
Abstract
BACKGROUND: Quality of cardiovascular disease (CVD) preventive care is suboptimal. Recent data correlated increasing years in practice for physicians with lower-quality health care.
OBJECTIVE: The purpose of this study was to assess physician awareness/adherence to national blood pressure, cholesterol, and CVD prevention guidelines for women according to physician/practice characteristics.
DESIGN: Standardized online survey and experimental case studies were administered to 500 randomly selected U.S. physicians. Multivariable regression models tested physician age, gender, specialty, and practice type as independent predictors of guideline awareness/adherence.
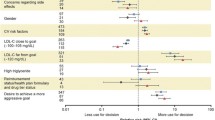
RESULTS: Compared with older physicians (50+ years), younger physicians (<50 years) reported a lower level of awareness of cholesterol guidelines (P=.04) and lower incorporation of women’s guidelines (P=.02). Yet, older physicians were less likely to recommend weight management for high-risk cases (P=.03) and less confident in helping patients manage weight (P=.045) than younger physicians. Older physicians were also less likely to identify a low-density lipoprotein <100 mg/dL as optimal versus younger physicians (P=.01), as were solo versus nonsolo practitioners (P=.02). Solo practitioners were less aware of cholesterol guidelines (P=.04) and were more likely to prescribe aspirin for low-risk female patients than nonsolo practitioners (P<.01). Solo practitioners rated their clinical judgment as more effective than guidelines in improving patient health outcomes (P<.01) and more frequently rated the patient as the greatest barrier to CVD prevention versus nonsolo practitioners (P<.01).
CONCLUSIONS: Though guideline awareness is high, efforts to promote their utilization are needed and may improve quality outcomes. Targeted education and support for CVD prevention may be helpful to older and solo physicians.
Similar content being viewed by others

References
American Heart Association. Heart disease and stroke statistics—2005 update. Dallas, Texas: American Heart Association; 2005. Accessed from: http://www.americanheart.org. May 19, 2005.
Mosca L, Manson JE, Sutherland SE, Langer RD, Manolio T, Barrett-Connor E. Cardiovascular disease in women: a statement for healthcare professionals from the American Heart Association. Writing Group. Circulation. 1997;96:2468–82.
Kim C, Hofer TP, Kerr EA. Review of evidence and explanations for suboptimal screening and treatment of dyslipidemia in women. A conceptual model. J Gen Intern Med. 2003;18:854–63.
Sueta CA, Chowdhury M, Boccuzzi SJ, et al. Analysis of the degree of undertreatment of hyperlipidemia and congestive heart failure secondary to coronary artery disease. Am J Cardiol. 1999;83:1303–7.
Pearson TA, Laurora I, Chu H, Kafonek S. The lipid treatment assessment project (L-TAP): a multicenter survey to evaluate the percentages of dyslipidemic patients receiving lipid-lowering therapy and achieving low-density lipoprotein cholesterol goals. Arch Intern Med. 2000;160:459–67.
Ford ES, Mokdad AH, Giles WH, Mensah GA. Serum total cholesterol concentrations and awareness, treatment, and control of hyperocholesterolemia among US adults: findings from the National Health and Nutrition Examination Survey, 1999 to 2000. Circulation. 2003;107:2185–9.
Jha A, Varosy PD, Kanaya AM, et al. Differences in medical care and disease outcomes among black and white women with heart disease. Circulation. 2003;108:1089–94.
CDC. Missed opportunities in preventive counseling for cardiovascular disease—United States 1199099991995. Morb Mortal Wkly Rep. 1998;47:91–5.
Mosca L, Appel LJ, Benjamin EJ, et al. Evidence-based guidelines for cardiovascular disease prevention in women. Circulation. 2004;109:672–93.
Third Report of the National Cholesterol Education Program (NCEP) Expert Panel on Detection, Evaluation, and Treatment of High Blood Cholesterol in Adults (Adult Treatment Panel III) Final Report. National Cholesterol Education Program (NCEP) Expert Panel on Detection, Evaluation, and Treatment of High Blood Cholesterol in Adults (Adult Treatment Panel III). Circulation. 2002;106:3143–21.
Chobanian AV, Bakris GL, Black HR, et al. National Heart, Lung, and Blood Institute Joint National Committee on Prevention, Detection, Evaluation, and Treatment of High Blood Pressure; National High Blood Pressure Education Program Coordinating Committee. The seventh report of the joint national committee on prevention, detection, evaluation, and treatment of high blood pressure: the JNC 7 report. JAMA. 2003;289:2560–72.
Choudhry NK, Fletcher RH, Soumerai SB. Systematic review: the relationship between clinical experience and quality of health care. Annals Intern Med. 2005;142:260–73.
Mosca L, Linfante AH, Benjamin EJ, et al. National study of physician awareness and adherence to cardiovascular disease prevention guidelines. Circulation. 2005;111:499–510.
Castaldo J, Nester J, Wasser T, et al. Physician attitudes regarding cardiovascular risk reduction: the gaps between clinical importance, knowledge, and effectiveness. Dis Manag. 2005;8:93–105.
Galuska DA, Will JC, Serdula MK, Ford EA. Are health care professional advising obese patients to lose weight? JAMA. 1999;282:1576–8.
Yanovski SZ, Yanovski JA. Obesity. N Engl J Med. 2022;346:591–602.
Tsui JI, Dodson K, Jacobson TA. Cardiovascular disease prevention counseling in residency: resident and attending physician attitudes and practices. J Natl Med Assoc. 2004;96:1080–3.
Grundy SM, Cleeman JI, Bairey Merz CN, et al. Implications of recent clinical trials for the National Cholesterol Education Program Adult Treatment Panel III Guidelines. Circulation. 2004;110:227–39.
Ridker PM, Cook NR, Lee IM, et al. A randomized trial of low-dose aspirin in the primary prevention of cardiovascular disease in women. N Engl J Med. 2005;352:1293–304.
Willison DJ, Soumerai SB, Palmer RH. Association of physician age and hospital volume with use of aspirin and reperfusion therapy in acute myocardial infarction. Med Care. 2000;38:1092–102.
Beaulieu MD, Blais R, Jacques A, Battista RN, Lebeau R, Brophy J. Are patients suffering from stable angina receiving optimal medical treatment? QJM. 2001;94:301–8.
Fehrenbach SN, Budnitz DS, Gazmararian JA, Krumholz HM. Physician characteristics and the initiation of beta-adrenergic blocking agent therapy after acute myocardial infarction in a managed care population. Am J Manag Care. 2001;7:717–23.
Mehta RH, Montoye CK, Gallogly M, et al. Improving quality of care for acute myocardial infarction: The Guidelines Applied in Practice (GAP) Initiative. JAMA. 2002;287:1269–76.
Wolff M, Bower DJ, Marbella AM, Cassanova JE. US family physicians’ experiences with practice guidelines. Fam Med. 1998;30:117–21.
Freiman MP. The rate of adoption of new procedures among physicians. The impact of specialty and practice characteristics. Med Care. 1985;23:939–45.
James PA, Cowan TM, Graham RP, Majeroni BA. Family physicians’ attitudes about and use of clinical practice guidelines. J Fam Practice. 1997;45:341–7.
Author information
Authors and Affiliations
Corresponding author
Additional information
The authors have no conflicts of interest to report.
This research was partially funded by an unrestricted educational grant to the American Heart Association from KOS Pharmaceuticals. A National Institutes of Health training grant provided funding for Dr. Allison Christian to work on this study. Everyone who has contributed significantly to this work has been acknowledged.
Rights and permissions
About this article
Cite this article
Christian, A.H., Mills, T., Simpson, S.L. et al. Quality of cardiovascular disease preventive care and physician/practice characteristics. J Gen Intern Med 21, 231–237 (2006). https://doi.org/10.1111/j.1525-1497.2006.00331.x
Received:
Revised:
Accepted:
Issue Date:
DOI: https://doi.org/10.1111/j.1525-1497.2006.00331.x