


A 45-year-old man from Paraguay, South America, was referred to our dermatology department in Spain because of a 6-month history of nonpruriginous lesions that were unresponsive to local or oral corticosteroid treatment. He had been living in Spain for 4 years. Examination showed symmetric, annular or homogeneous erythematous plaques on his trunk and extremities (Figure 1). We suspected Hansen disease (leprosy) because the lesions showed a loss of sensation toward light touch and pin prick. A skin biopsy showed dermal perineural granulomatous inflammation and scarce mycobacterium after Ziehl–Neelsen staining, and polymerase chain reaction showed the presence of Mycobacterium leprae (Appendix 1, available at www.cmaj.ca/lookup/suppl/doi:10.1503/cmaj.130221/-/DC1). Multibacillary leprosy was diagnosed, and therapy with dapsone, rifampin and clofazimine was initiated. Physical examination of the other members of the family was negative.
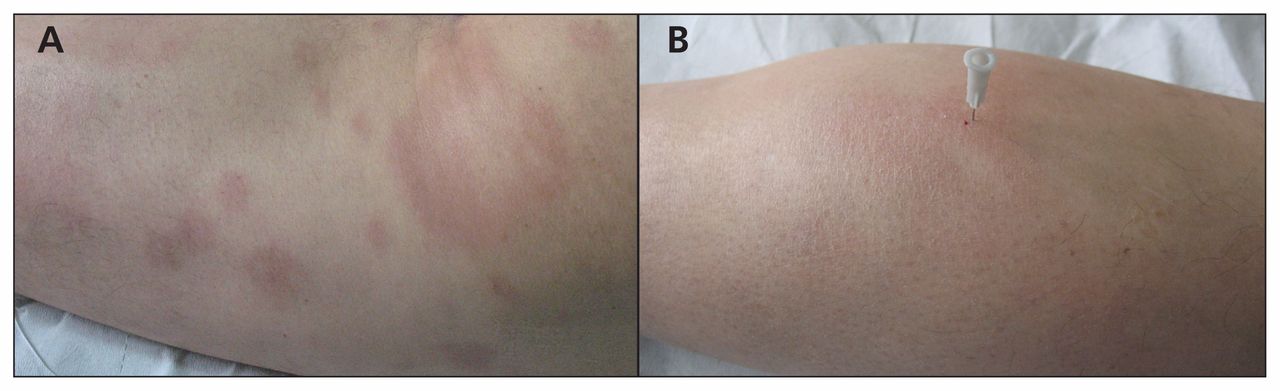
(A) Symmetric, annular or homogeneous erythematous plaques on the trunk and extremities of a 45-year-old man with Hansen disease (leprosy). (B) The lesions showed a loss of sensation toward light touch and pin prick.
The global prevalence of leprosy has decreased substantially, but transmission continues in a few areas. Over 228 000 new cases were reported in 2010, mainly in India and Brazil.1 The diagnosis may be delayed in developed countries,2 but it should be considered for those coming from areas in which leprosy is endemic, taking into account the long incubation period (2–12 yr).3
According to the World Health Organization, an individual living in an area in which leprosy is endemic should be regarded as having leprosy if at least 1 of the following signs is present: skin lesion(s) consistent with leprosy and sensory loss; or positive skin smears.4 The lesions may be macules, papules, annular plaques or nodules. Loss of sensation to pin prick and light touch is a typical feature. Peripheral thickened nerves with signs of neural damage, including muscle weakness, may also be seen.4
Microbiological cultures are not available for leprosy. The identification of leprosy bacilli by use of special stains is indicative of multibacillary leprosy. The absence of leprosy bacilli is indicative of paucibacillary leprosy.4 The choice of therapy depends on the classification of leprosy, with dapsone, rifampin and clofazimine recommended for multibacillary leprosy, and dapsone and rifampin recommended for paucibacillary leprosy.3
Footnotes
-
See also the practice article by Tremblay and Albert on page 206 and at www.cmaj.ca/lookup/doi/10.1503/cmaj.130688
-
This article has been peer reviewed.
-
Competing interests: None declared.
In this issue

{kind=link}
Article tools






Related Articles
Cited By...
- No citing articles found.
More in this TOC Section
Similar Articles
Collections

