

A 64-year-old woman of Asian descent presented to the emergency department with an initial diagnosis of hyperosmolar hyperglycemic state. She had type 2 diabetes mellitus and cervical cancer, and had received chemotherapy with cisplantin 3 days before presentation.
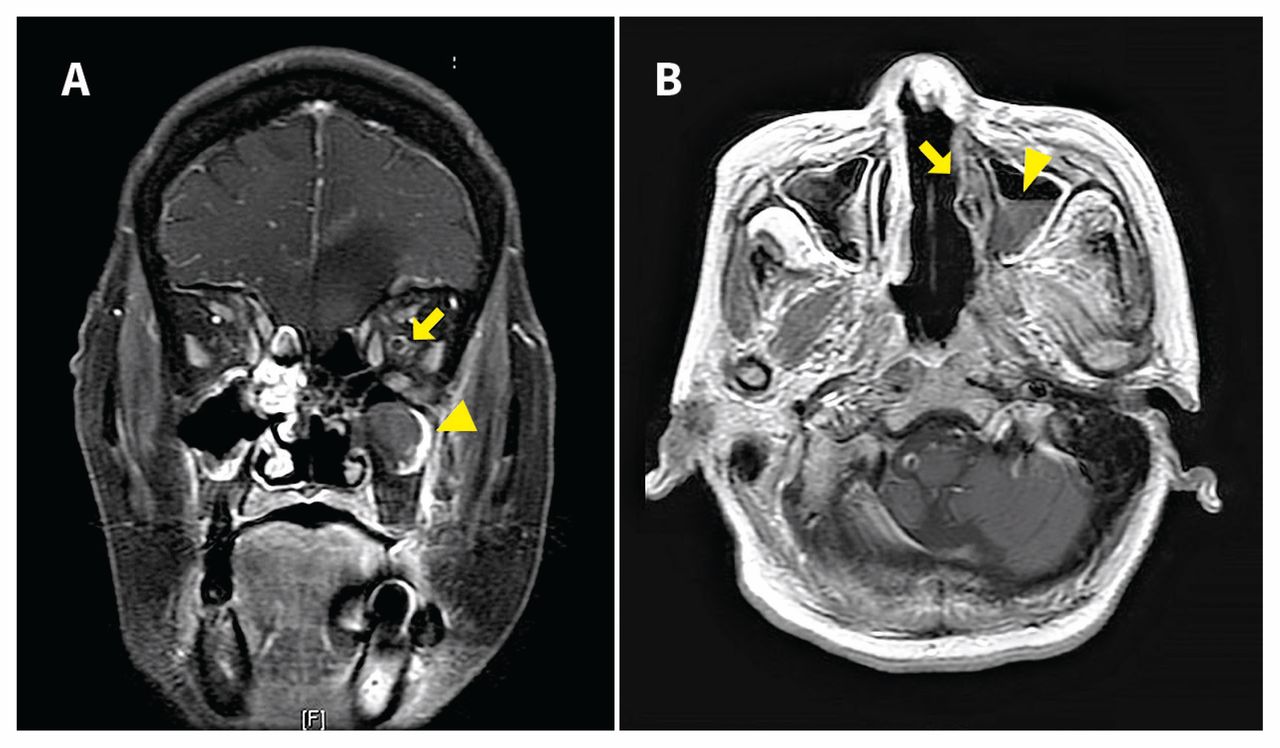
On being admitted to hospital, the patient experienced sudden-onset blindness, and chemosis and proptosis of the left eye, accompanied by low-grade fever (38.2°C). Postcontrast T1-weighted magnetic resonance imaging (MRI) showed hypointensity in her left frontal lobe and enhancement around her left optic nerve, indicating perineuritis (Figure 1A). In addition, on diffusion-weighted imaging, hyperintensity in her left optic nerve (Appendix 1A, available at www.cmaj.ca/lookup/suppl/doi:10.1503/cmaj.181210/-/DC1) with decreased apparent diffusion coefficient (Appendix 1B) indicated acute infarction. The presence of a black turbinate sign in her left nasal cavity, and an air-fluid level over her left maxillary sinus was consistent with infective sinusitis (Figure 1B).
{kind=link}
(A) Coronal T1-weighted contrast-enhanced magnetic resonance image (MRI) showing hypointensity in the left frontal lobe of the brain of a 64-year-old woman, indicating ischemic infarction, enhancement around, rather than within, the left optic nerve with doughnut appearance (arrow), indicating perineuritis, and mucosal thickening in the left maxillary sinus (arrowhead). (B) Axial view showing lack of enhancement of the left nasal turbinate (black turbinate sign, arrow) and an air-fluid level over her left maxillary sinus (arrowhead), indistinguishable from that seen in bacterial sinusitis.
We performed urgent surgical débridement, noting eschar formation over the patient’s left nasal cavity with bone erosion (Appendix 1C). Results from histologic examination showed broad and nonseptated fungal hyphae at 90° angles, confirming mucormycosis. Despite treatment with amphotericin B, the patient died 2 weeks later.
Mucormycosis is an uncommon but fatal fungal infection, found in 10% of all fungal infections at autopsy and primarily affecting patients who are immunocompromized, especially those with diabetes.1 Early diagnosis and treatment are crucial for survival. The sinuses are most commonly affected, and subsequent rhino-orbital-cerebral mucormycosis is closely associated with diabetes.1 A clinical presentation of orbital swelling, black nasal discharge, visual defect, proptosis and headache suggests rhinoorbital-cerebral mucormycosis.1 Black turbinate sign represents devitalized mucosa leading to a hypointense mucosal appearance on MRI. There is a previous report of a patient who developed nerve infarction 2 weeks after being diagnosed with mucormycosis; 2 optic neuritis and infarction as the initial presentation of mucormycosis is uncommon.3 Contrast-enhanced MRI can show the spread of perineural infection as high signal intensity along the nerve3 and is more valid than computed tomography.1
Footnotes
Competing interests: None declared.
This article has been peer reviewed.
The authors have obtained consent from the patient’s daughter.