

Abstract
Background: Escherichia coli O157:H7 is one cause of acute bacterial gastroenteritis, which can be devastating in outbreak situations. We studied the risk of cardiovascular disease following such an outbreak in Walkerton, Ontario, in May 2000.
Methods: In this community-based cohort study, we linked data from the Walkerton Health Study (2002–2008) to Ontario’s large healthcare databases. We included 4 groups of adults: 3 groups of Walkerton participants (153 with severe gastroenteritis, 414 with mild gastroenteritis, 331 with no gastroenteritis) and a group of 11 263 residents from the surrounding communities that were unaffected by the outbreak. The primary outcome was a composite of death or first major cardiovascular event (admission to hospital for acute myocardial infarction, stroke or congestive heart failure, or evidence of associated procedures). The secondary outcome was first major cardiovascular event censored for death. Adults were followed for an average of 7.4 years.
Results: During the study period, 1174 adults (9.7%) died or experienced a major cardiovascular event. Compared with residents of the surrounding communities, the risk of death or cardiovascular event was not elevated among Walkerton participants with severe or mild gastroenteritis (hazard ratio [HR] for severe gastroenteritis 0.74, 95% confidence interval [CI] 0.38–1.43, mild gastroenteritis HR 0.64, 95% CI 0.42–0.98). Compared with Walkerton participants who had no gastroenteritis, risk of death or cardiovascular event was not elevated among participants with severe or mild gastroenteritis.
Interpretation: There was no increase in the risk of cardiovascular disease in the decade following acute infection during a major E. coli O157:H7 outbreak.
Escherichia coli O157:H7 is one cause of acute bacterial gastroenteritis, causing 63 000 infections each year and 12 major outbreaks since 2006 in the United States alone.1,2 This strain was most recently implicated in the outbreak involving beef from XL Foods (September 2012), with 17 confirmed cases across Canada.3 A similar enterohemorrhagic strain E. coli O104:H4 was responsible for an outbreak in Germany in May 2011, causing 3792 cases of gastroenteritis and 43 deaths.4,5
Most patients fully recover from acute gastroenteritis caused by E. coli. However, such an illness may predispose patients to long-term disease. Shiga toxin is produced by E. coli O157:H7; this toxin damages the microvasculature of the kidneys leading to hypertension6–13 and directly damages the systemic vasculature.14–16 Infected people may progress from a state of acute inflammation of the vasculature to subclinical chronic inflammation, which could promote atherosclerosis.17–20
In Walkerton, Ontario, in May 2000, heavy rains transported bovine fecal matter into the town’s well, contaminating the inadequately chlorinated municipal water supply with E. coli O157:H7.21 Over 2300 people developed acute gastroenteritis, and 7 people died.22 The unique circumstances of this outbreak provided a rare opportunity to study the natural history following exposure to this pathogen in a single cohort.23 Other outbreaks have been geographically dispersed, making it difficult to track cases.24,25
In Walkerton, affected individuals were followed annually in a clinic to assess their long-term outcomes (Walkerton Health Study, 2002–2008). We previously reported that adults who experienced acute gastroenteritis during the outbreak had a higher than expected incidence of hypertension, chronic kidney disease and self-reported cardiovascular disease in follow-up.23 However, 46% of participants were lost to follow-up by the end of the study, and there were limitations associated with the assessment of cardiovascular disease by participant recall. Thus, we conducted an expanded and extended follow-up study, linking the Walkerton study data to Ontario’s health care databases. Our objective was to more accurately determine the 10-year risk of major cardiovascular events after exposure to E. coli O157:H7.
Methods
Design, setting and population
In this community-based cohort study, we linked data from the Walkerton Health Study to Ontario’s health care databases. We previously found that the Walkerton study cohort and the Walkerton population were demographically similar, aside from a slight overrepresentation of women and a slight underrepresentation of elderly people in the Walkerton study cohort.26 Population sampling and other methodologic details for the Walkerton Health Study are provided elsewhere.23,27
The date of enrollment in the Walkerton study was the first day of follow-up, referred to as the index date (Jan. 3, 2002, to Dec. 11, 2002). In the current study, we included 4 groups of adults aged 40–89 years on the index date: 3 groups were from the Walkerton study (adults with no, mild or severe gastroenteritis during the outbreak) and 1 control group comprised of residents from the surrounding communities that were unaffected by the outbreak. Validated criteria were used to assess illness severity (presence and duration of diarrheal illness, bloody diarrhea, abdominal pain, fever or positive stool culture for E. coli O157:H7).28 Self-reported illness was confirmed by medical-record audit when possible.28
For the control group, we considered residents of geographically proximal towns that were demographically similar to Walkerton (population 4851 in 2001;29 Appendix 1, available at www.cmaj.ca/lookup/suppl/doi:10.1503/cmaj.112161/-/DC1). This comparison group was created entirely from provincial health care databases, which contained relevant baseline data for the entire population of these communities (all Ontario residents have universal access to hospital and physician services).
Residents of the surrounding communities were randomly assigned an index date according to the distribution of such dates among the Walkerton participants. We applied the same eligibility criteria (Appendix 2, available at www.cmaj.ca/lookup/suppl/doi:10.1503/cmaj.112161/-/DC1) to all groups (Figure 1).

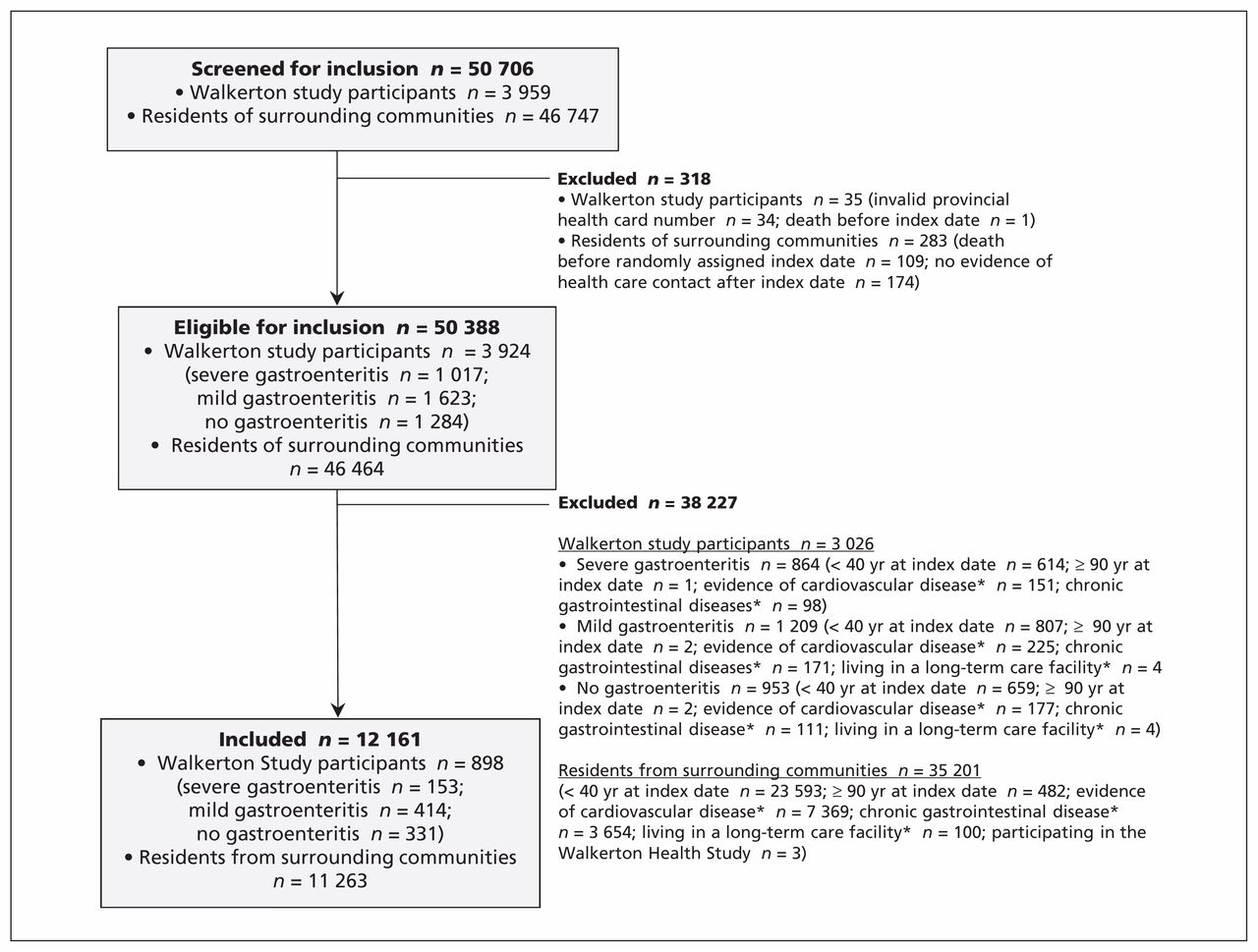{kind=link}
Selection of participants for inclusion in the study. *From Jan. 1, 1991, to May 17, 2000.
We excluded people with a history of chronic gastrointestinal disease before the outbreak (Jan. 1, 1991 to May 17, 2000) because assessment of acute gastroenteritis during the outbreak would be unreliable. We also excluded people with evidence of a previous cardiovascular event, hemolytic uremic syndrome or who lived in a long-term care facility before the index date.
All participants were followed from their index date until Mar. 31, 2010 (10 yr after the outbreak), death or emigration from the province.
Data sources
We used multiple databases to determine the cohorts, baseline characteristics and outcomes. The dataset from the Walkerton Health Study contains information on acute illness during the outbreak.28 The Canadian Institute for Health Information’s Discharge Abstract Database contains diagnostic and procedural information for all hospital admissions in Ontario. The Ontario Health Insurance Plan database contains all claims for inpatient and outpatient physician services, and the Ontario Registered Persons Database contains demographic and vital status information for all Ontario residents.30 The databases and the linked dataset were held securely in a deidentified form and were analyzed at the Institute for Clinical Evaluative Sciences. These databases have been used extensively in population-based health outcomes research and are essentially complete for the study variables.31–35
Outcomes
The primary outcome was a composite of death or first major cardiovascular event (admission to hospital for acute myocardial infarction, stroke or congestive heart failure, or procedures such as coronary artery bypass graft surgery, coronary angioplasty, carotid endarterectomy, abdominal aortic aneurysm repair, aortic bypass or peripheral vascular bypass surgery) as defined using validated codes in Appendix 3 (available at www.cmaj.ca/lookup/suppl/doi:10.1503/cmaj.112161/-/DC1).36–44 The secondary outcome was first major cardiovascular event censored for death.
Statistical analysis
We compared baseline characteristics (Appendix 4, available at www.cmaj.ca/lookup/suppl/doi:10.1503/cmaj.112161/-/DC1) across the 4 groups using analysis of variance, Kruskal–Wallis or χ2 tests as appropriate. We included age (per yr) and sex in all multivariable models. We retained the following variables if their inclusion changed the associate between acute gastroenteritis and cardiovascular disease by more than 5%:45–49 socioeconomic status (assessed by use of neighbourhood income quintile, a household size–adjusted measure of income),50 a measure of comorbidity (Johns Hopkins Aggregated Diagnosis Groups),51 diabetes, chronic obstructive pulmonary disease or hypercholesterolemia at the index date, number of physician visits in the 2 years before the outbreak, and presence of hypertension or chronic kidney disease before the outbreak. We used a Cox proportional hazard regression model to calculate hazard ratios (HRs) and 95% confidence intervals (CIs). For the primary analysis, adults from surrounding communities served as the reference group. We confirmed the proportionality assumption using a time-dependent interaction.52
Results
Baseline characteristics
Our cohort included 898 people from the Walkerton Health Study (153 with severe gastroenteritis, 414 with mild gastroenteritis and 331 with no gastroenteritis during the outbreak) and 11 263 residents of surrounding communities (Figure 1). Compared with the Walkerton participants, residents of the surrounding communities were slightly older, more likely to be male and have fewer comorbidities, and they were less likely to be in the middle socioeconomic class. Those who experienced severe gastroenteritis during the outbreak were more likely than residents of surrounding communities to have had chronic kidney disease and to have had more visits to their family physician before the outbreak (Table 1). Of the 12 161 adults in this study, only 285 (2.3%) were lost to follow-up over an average of 7.4 years (1.1% of the Walkerton participants and 2.4% of the residents of surrounding communities).
Baseline characteristics of included participants from the Walkerton Health Study and from the surrounding communities.
Outcomes
There were 1174 deaths or major cardiovascular events during the study period: 1115 (9.9%) among residents of surrounding communities; 28 (8.5%) among those who had no gastroenteritis; 22 (5.3%) among those who had mild gastroenteritis; and 9 (5.9%) among those who had severe gastroenteritis (Table 2). Overall, there were 563 major cardiovascular events: 536 (4.8%) among residents of surrounding communities, 8 (2.4%) among those who had no gastroenteritis, 13 (3.1%) among those who had mild gastroenteritis, and 6 (3.9%) among those who had severe gastroenteritis. Compared with residents of surrounding communities, the adjusted hazard ratio for death or major cardiovascular event was not elevated among those with severe gastroenteritis during the outbreak (HR 0.74 [95% CI 0.38–1.43]), and the hazard ratio was significantly decreased among those with mild gastroenteritis (HR 0.64 [95% CI 0.42–0.98]). Similar patterns were seen for death-censored cardiovascular events (severe: HR 1.04 [95% CI 0.46–2.33]; mild: HR 0.75 [95% CI 0.43–1.30]) and death from all causes (severe: HR 0.39 [95% CI 0.13–1.21], mild: HR 0.52 [95% CI 0.29–0.97]).
Death and major cardiovascular events during the study period among people who experienced mild gastroenteritis (n = 414), severe gastroenteritis (n = 153) or no gastroenteritis (n = 331) during the Escherichia coli O157:H7 outbreak and among a control population (n = 11 263) from the surrounding communities
Additional planned analyses
We repeated the above analyses using only Walkerton study participants. In this analysis, we considered adults who had no gastroenteritis during the outbreak to be the reference group (Table 3). Additional baseline characteristics, including objective measures of kidney function (serum creatinine, urine protein, urine albumin/creatinine ratio) at the index date were not different between the 3 groups (Appendix 5, available at www.cmaj.ca/lookup/suppl/doi:10.1503/cmaj.112161/-/DC1). The hazard for death or major cardiovascular events was not elevated among Walkerton participants with severe or mild gastroenteritis during the outbreak compared with Walkerton participants with no symptoms (severe: HR 0.75 [95% CI 0.35–1.59]); mild: HR 0.63 [95% CI 0.36–1.10]).
Death or major cardiovascular event after Escherichia coli O157:H7 gastroenteritis among participants in the Walkerton Health Study with no gastroenteritis (n = 331), mild gastroenteritis (n = 414) or severe gastroenteritis (n = 153)
Post-hoc analyses
Health care surveillance in Walkerton intensified in response to the outbreak through extra physician clinics focused on hypertension control. Angiotensin-converting enzyme (ACE) inhibitors and angiotensin receptor blockers (ARBs) were preferentially prescribed given concerns about the long-term renal effects of E. coli O157:H7. To examine whether differential health care played a role in preventing outcomes, we compared the proportion of prescriptions for antihypertensive medications in the years before and after the study (Appendix 6, available at www.cmaj.ca/lookup/suppl/doi:10.1503/cmaj.112161/-/DC1). We restricted this analysis to those aged 66 to 76 because prescription drug coverage is a universal benefit to Ontarians aged 65 years and older.
The overall rates of antihypertensive prescriptions were similar between the general population and Walkerton participants in 1999 (28% v. 30%, respectively) and 2009 (53% v. 52%, respectively). Between 1999 and 2009, prescriptions for ACE inhibitors or ARBs rose from ≤ 7% to 34% among Walkerton participants and from 14% to 40% among residents of surrounding communities.
To contrast the results of the current study with those from our previous report, which described cardiovascular events assessed by participant recall, we compared self-reported cardiovascular events and events documented in the health care databases. Most (81%) of the hospitalizations for a cardiovascular event captured in Ontario databases were also reported by Walkerton study participants; however, only 57% of self-reported cardiovascular events were corroborated by database codes for cardiovascular-related hospitalization (data not shown). Differential reporting by severity of gastroenteritis was not evident.
Interpretation
We found that the 10-year risk for cardiovascular disease was not higher among adults who had severe gastroenteritis and was actually lower among those who had mild gastroenteritis during an E. coli O157:H7 outbreak.
We previously found increased risks of hypertension, chronic kidney disease and self-reported cardiovascular disease among adults who experienced acute gastroenteritis after drinking water contaminated with E. coli O157:H7.23,27 Although we used objective, standardized measures to diagnose hypertension and chronic kidney disease, our previous study relied on participant recall of major cardiovascular events, and there was significant loss to follow-up. This prompted us to conduct a more accurate assessment of cardiovascular risk by linking data from the Walkerton Health Study to Ontario’s health care databases, allowing the use of administrative codes to determine outcomes, which is more reliable than self-report. Only 57% of self-reported cardiovascular events were corroborated by validated database codes for cardiovascular-related hospitalization. No association between acute gastroenteritis and cardiovascular-related events was evident.
These discrepant results suggest 2 possible scenarios: either there is no causal link between E. coli O157:H7 gastroenteritis and cardiovascular events, or an association exists but we were unable to detect it in the present study. Despite the robust association with hypertension,23,27 it is possible that the biological mechanisms thought to link E. coli O157:H7 and cardiovascular disease are inadequate to precipitate major cardiovascular events — or perhaps 10 years is not long enough for such events to manifest. Alternatively, by virtue of participating in the Walkerton study, participants received extra health care and screening for hypertension and kidney disease.53 These risk factors for cardiovascular disease are asymptomatic and often go untreated in the absence of active surveillance, so diagnosis and treatment of these conditions may have been greater for Walkerton participants compared with their unexposed counterparts in the surrounding communities.
Among Walkerton participants with hypertension, the proportion receiving treatment increased from 18% to 77% during follow-up, and the overall proportion with elevated systolic/diastolic blood pressure (> 140/90 mm Hg) decreased from 25% to 20%.53 To examine this further, we compared the rates of antihypertensive prescription use before and after the study among those with provincial drug benefits. Overall rates of antihypertensive prescriptions were similar between groups at both time points; however, between 1999 and 2009, an 8-fold rise in prescriptions for ACE inhibitors or ARBs among Walkerton participants occurred (≤ 7% to 34%), compared with a 3-fold rise among residents of surrounding communities (14% to 40%). Although prescription rates were not appreciably different in 2009, it is possible that the greater relative increase in ACE or ARB use among Walkerton participants played a role in preventing cardiovascular disease among study participants.
Strengths and limitations
Our study examined long-term health outcomes after acute bacterial gastroenteritis caused by E. coli O157:H7 in a well-defined cohort with minimal loss to follow-up (2.3%). All outcomes were measured using validated codes with high specificities and positive predictive values.36–44 The method of determining acute gastrointestinal illness at the time of the outbreak was validated using both public health and medical records.28 Although we could not reliably determine the cause of death from our data sources, cardiovascular disease is a leading cause of death in Ontario, with an age-adjusted mortality of 29%.54 To protect against potential immortal-time bias,55 we excluded cardiovascular events between the outbreak and each participant’s index date (enrollment in the Walkerton study).55,56 There was no appreciable difference in the proportion excluded for this reason across comparison groups (1.75% of eligible participants).
As in other outbreak situations, multiple bacteria contaminated the water; Campylobacter jejuni was also detected, and coinfection occurred. It is possible that exposure misclassification could have attenuated the association, if one exists. However, because the infectious dose of E. coli O157:H7 is much lower than that of Campylobacter (10–100 cells v. 500–10 000 cells),1 it is unlikely that a participant with acute gastroenteritis was unexposed to E. coli O157:H7.
It is possible that the apparent protective association between mild illness and cardiovascular disease could have resulted from unmeasured or residual confounding if those who suffered only mild illness after infection with E. coli O157:H7 were selectively healthier than the average individual.
Finally, because of the observational nature of the study, we can only establish the lack of an association and not the lack of a causal relation. Nonetheless, the contamination of Walkerton’s municipal water was a disastrous event in a well-defined population, and we controlled for many confounders using exclusions and statistical adjustments. Additionally, the absence of an elevated risk was consistent across all outcomes; unadjusted hazard ratios were either nonsignificant or less than one. This strongly supports our findings of no increased risk of cardiovascular events or death in this population.
Conclusion
This study provides evidence that the risk of major cardiovascular events was not higher in Walkerton in the decade following the E. coli O157:H7 outbreak. This may be partly explained by active surveillance and treatment for conditions such as hypertension, which may prevent cardiovascular events.
Footnotes
Competing interests: William Clark and Amit Garg have provided medical expert testimony on hemolytic uremic syndrome in the United States. None declared by all other authors.
This article has been peer reviewed.
Contributors: All authors contributed to the study design, data collection and analysis, interpretation, and writing and revising the manuscript. All of the authors approved the final version submitted for publication.
Funding: This study was supported by the Institute for Clinical Evaluative Sciences (ICES), which is funded by an annual grant from the Ontario Ministry of Health and Long-Term Care (MOHLTC). The opinions, results and conclusions reported in this paper are those of the authors and are independent from the funding sources. No endorsement by ICES or MOHLTC is intended or should be inferred.
The Walkerton Health Study was funded by the Ontario Ministry of Health. The current project was funded by the Canadian Institutes of Health Research. Patricia Hizo-Abes was supported by a Summer Research Training Program grant, the Heart and Stroke Foundation and the Mach-Gaensslen Foundation of Canada. Peter Austin was supported in part by a Career Investigator Award from the Heart and Stroke Foundation of Ontario. Amit Garg was supported by a Canadian Institutes of Health Research Clinician–Scientist Award. The opinions, results and conclusions reported in this paper are those of the authors and are independent of the funding sources.
Members of the Walkerton Health Study Investigators: Drs. Stephen Collins, John Howard, Douglas Matsell, John Marshall, Jennifer Macnab, Louise Moist, Janet Pope, Marina Salvadori and Rita Suri.