

The last time Canada’s medical education system underwent a comprehensive review, Wilfred Laurier was prime minister and the Ottawa Hockey Club nabbed the Stanley Cup from the Montréal Wanderers. That was in 1910, when Abraham Flexner, an American education expert, wrote a report that transformed medical education in Canada and the United States.
Now, a century later, the Association of Faculties of Medicine of Canada has taken another look at medical education in Canada and, as expressed in a new report, has found that it is again time for change.
“The timeliness of this report cannot be overstated,” Dr. Nick Busing, president and chief executive officer of the Association of Faculties of Medicine of Canada, told an audience gathered in Ottawa, Ontario, on Jan. 28 for the report’s official launch. A lot has changed in medical practice in recent decades, Busing noted, including a “virtual explosion” of scientific knowledge and incredible advances in medical technology.
In the report, The Future of Medical Education in Canada (FMEC): A Collective Vision for MD Education, the association makes 15 recommendations on how to improve medical education to meet the increasingly complex and diverse needs of Canadians (www.afmc.ca/fmec/pdf/collective_vision.pdf). The recommendations address such things as medical school admissions, the social accountability of physicians and the need to train doctors to be part of interprofessional teams (for a full list, see Box 1).
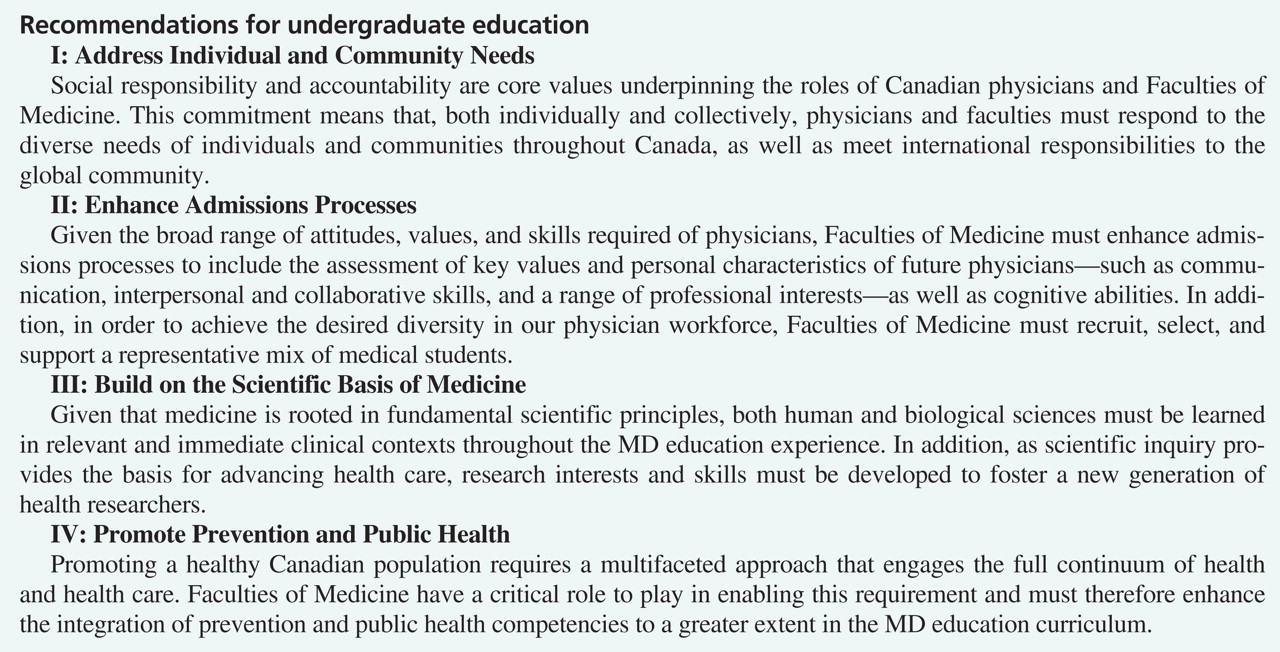
Box I: The Association of Faculties of Medicine’s MD education project’s full recommendations:

BOX. No caption available.
“Simply put, this report identifies both generally agreed upon and uniquely Canadian challenges in MD education and offers a transformative vision for the way forward,” the report states. “It strikes a balance between the impetus for change, what is currently being done, and what remains to be done.”

{kind=link}
{kind=link}
{kind=link}
The training of physicians should be extended beyond the medical classroom and teaching hospitals to include community clinic, rural hospitals and other medical facilities, the Association of Faculties of Medicine of Canada says. Image courtesy of © 2010 Jupiterimages Corp.
Though the ideas presented in the report aren’t new, the FMEC Collective Vision project, which started in 2007, is important because it is a national initiative, says Dr. Lewis Tomalty, vice-dean of medical education at Queen’s University in Kingston, Ontario. Canadian medical schools traditionally focus on improving education in areas most relevant to their regions, he says, but a country-wide vision was needed.
“I think the report has no actual surprises, but it captures conversations in areas we knew about and put them together,” Tomalty says. “What’s strong and exciting about this report is that it’s taking these things and putting them on paper. It will take a huge amount of work to implement these recommendations and it will not happen overnight, by any stretch, but it gives us something to move forward toward.”
At the top of the list of recommendations in the report is to better address community needs. Doctors must be concerned not only with delivering health care services but with being socially responsible and accountable.
“Social accountability is about our need to respond as medical institutions to societal needs in medicine,” says Tomalty. “It links directly into things like the fact that we have massive diversity in our population, from rural to urban, from the poor to the affluent.”
Another important aspect of medical education that needs to change is the admission process, the report states. Successful candidates for medical school should have more than good grades; their personal values and characteristics — such as communication and interpersonal skills — must also be considered. There is also a need to recruit and support a more diverse mix of students to reflect Canada’s diverse population.
“We need to be more inclusive,” says Tomalty, who notes that while medical students are more diverse in gender and race than in years past, they still primarily come from the same high socio-economic class. “How do we attract Aboriginal students?”
The report also highlights the need to educate doctors on how to work collaboratively instead of training them as, in Tomalty’s words, “isolated entities.” There is a move in Canadian health care toward collaborative, patient-centred care, the report states, and medical education should reflect the changes in medical practice, so that new doctors are equipped to work on teams.
The recommendations are the result of more than a year of literature review and analysis, and meetings with Canadian experts on medical education, as well as experts from other countries, such as New Zealand, the United Kingdom and the Netherlands. All 17 Canadian faculties of medicine were consulted on the recommendations after they were drafted.
The Association of Faculties of Medicine of Canada has high hopes for the report, but acknowledges that its effects on transforming medical education in Canada will depend on how medical schools implement the recommendations.
“The FMEC Collective Vision is a prescription for change,” the report concludes. “Individual faculties will, no doubt, address each of the recommendations in different ways by establishing priorities in accordance with community needs, faculty strengths, areas needing improvement, and visionary strategic directions for the 21st century. It will be the collective vision and its implementation, however, that truly result in transformative change.”
The report follows on the heels of an earlier call by the Association of American Medical Colleges, which represents all 130 US and the 17 accredited Canadian medical schools, to overhaul undergraduate and medical school curricula to focus on bolstering the scientific competency of doctors (CMAJ 2009. DOI:10.1503/cmaj.091197).
Footnotes
-
Published at www.cmaj.ca on Feb. 1