

Abstract
Background: The Ontario Maternal Serum Screening (MSS) Program was introduced by the Ontario Ministry of Health as a province-wide pilot project in 1993. The objective of this study was to determine the influence of practice location on Ontario health care providers' use of and opinions regarding MSS, access to follow-up services and recommendations about the program.
Methods: A questionnaire was mailed to a random sample of 2000 family physicians, all 565 obstetricians and all 62 registered midwives in Ontario between November 1994 and March 1995.
Results: Among providers who were eligible (those providing antenatal care or attending births) the response rates were 91.4% (778/851), 76.0% (273/359) and 78.0% (46/59) respectively. Fewer respondents in the Northwest region (71.4%) and in rural areas (81.9%) stated that they routinely offer MSS to all pregnant women in their practices compared with respondents in other regions (84.4%-91.5%) and urban centres (90.1%). Fewer respondents in the northern regions (Northeast 49.2%, Northwest 25.0%) than in the Central East region (includes Toronto) (76.6%) felt that follow-up services were readily available. Respondents in the northern regions had less favourable opinions of MSS than those in the other regions in terms of its complexity, cost, the time involved in counselling and the high false-positive rate. More respondents in the Central East region (64.6%) and in urban centres (52.9%) recommended not changing the MSS program than did those in the Northwest (7.1%) and rural areas (39.8%). After provider characteristics were controlled for in a logistic regression analysis, practice location was not the most important factor. Instead, the model showed that respondents who cared for 50 or more pregnant women in the previous year were more likely to offer MSS routinely (OR 2.00, 95% CI 1.21-3.27) and that those who felt that patient characteristics affect the offering of MSS (OR 0.42, 95% CI 0.26-0.67) or that follow-up services were not readily available (OR 0.33, 95% CI 0.20-0.55) were less likely to offer it.
Interpretation: Health care providers in northern and rural Ontario were less likely to offer MSS routinely than those in other regions and were more likely to recommend changing or eliminating the program. Providers' concerns about the social and cultural sensitivity of MSS and the availability of follow-up services affected use.
The Ontario Ministry of Health introduced the Ontario Maternal Serum Screening (MSS) Program as a province-wide pilot project on July 1, 1993. The intent of the program was that health care providers offer MSS to all pregnant women in their practices with appropriate counselling. Genetic counsellors and resources were available through regional genetic centres.
The purpose of MSS is to determine a pregnant woman's risk of carrying a fetus with Down syndrome, trisomy 18 or an open neural tube defect by measuring 3 serum markers: alpha-fetoprotein, human chorionic gonadotropin and unconjugated estriol. The detection rate of Down syndrome through MSS ranges from 48% to 91% (median 58%), [1] and the false-positive rate ranges from 3% to 7%. [1–5] Data from the first year of the Ontario MSS program showed a detection rate of 66% for Down syndrome, with a false-positive rate of 6%. [6] The sensitivity and specificity of MSS in detecting Down syndrome are reported as 91% and 94% respectively. [7] MSS can detect an estimated 85% of trisomy 18 cases [8] and approximately 80%-85% of open neural tube defects. [9]
In 1985 Manitoba introduced a province-wide prenatal genetic screening program using a single marker (alpha-fetoprotein). A 1992 survey revealed that family physicians and obstetricians in Winnipeg had more favourable opinions, were more informed and were more likely to offer the test than rural physicians, who had concerns about the cost of the test and the lack of follow-up services. [10]
A study in the Sioux Lookout Zone, a remote region in northwestern Ontario, found that MSS did not meet the needs of the mainly native Cree and Ojibway inhabitants and was not well received by the physicians in the region who provided antenatal care. [11] Difficulties in implementing the test included delays in receiving test results and the lack of follow-up services.
The purpose of this study was to determine the influence of practice location on Ontario health care providers' use of and opinions regarding MSS, access to follow-up services and recommendations about the program. We felt that a better understanding of regional differences might facilitate the future introduction of other province-wide genetic screening programs.
Methods
The survey's development, content and reliability are described elsewhere. [12] In brief, the sample included 2000 Ontario family physicians randomly selected from the membership list of the College of Family Physicians of Canada, all 565 obstetricians from a list provided by the Ontario Medical Association and all 62 registered midwives from a list provided by the College of Midwives of Ontario. The eligibility criterion was the current provision of antenatal care or attendance at births.
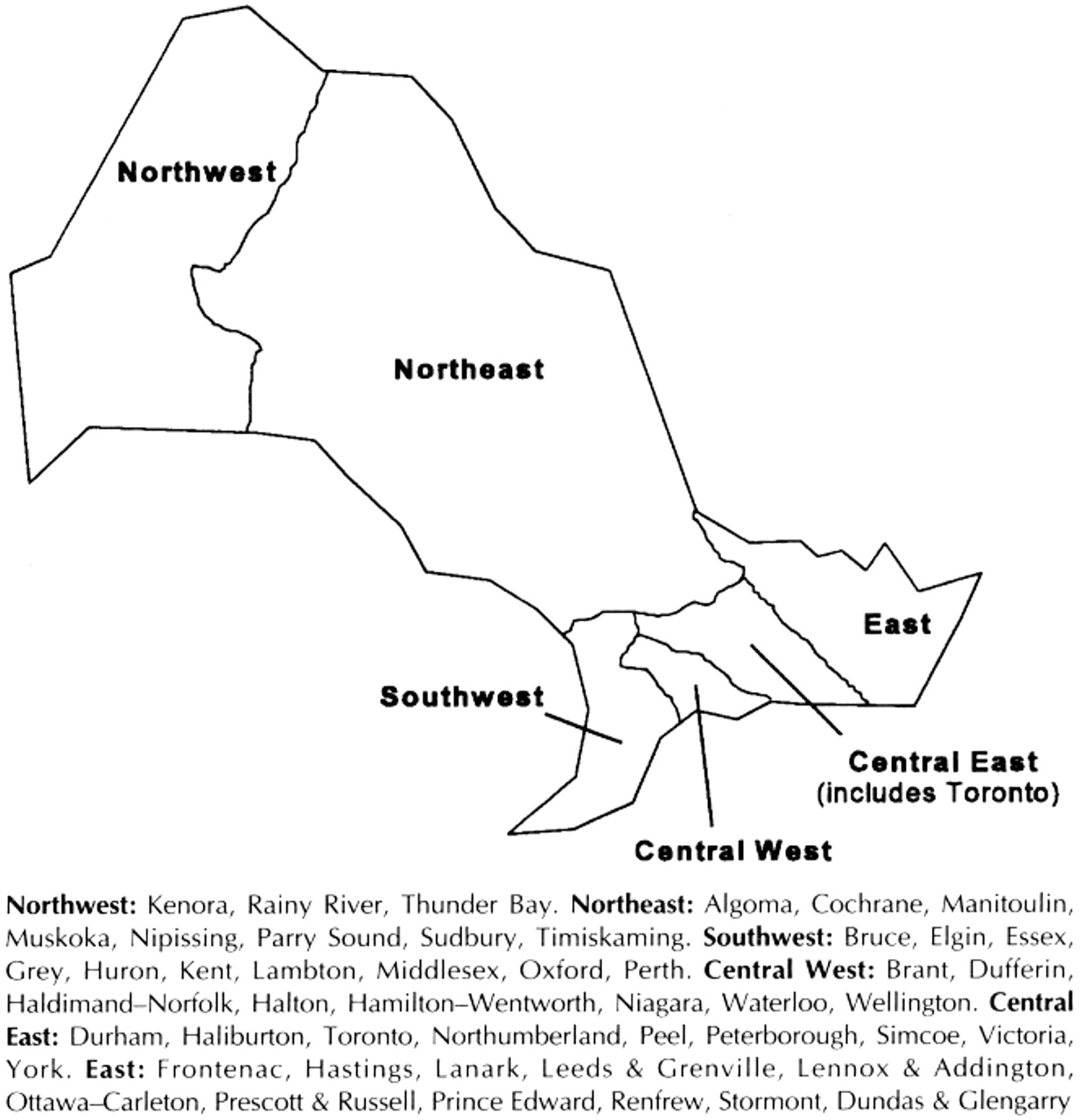
Health care providers who practised in communities with a population of 50 000 or less were classified as practising in a rural area. The Ontario Ministry of Health Residence Coding Manual [13] was used to code the various planning regions (Figure 1). The survey was conducted between November 1994 and March 1995; we used a modified Dillman technique. [14] A random sample of non-respondents received a telephone call to verify eligibility.

{kind=link}
Figure 1. Ontario Ministry of Health planning regions used in study to categorize respondents by practice location. (Regional areas outlined on map are approximate.)
Statistical comparisons were carried out using chi squared tests, t-tests and analysis of variance. Significant variables were entered into a multiple logistic regression model. In view of the multiple comparisons made, a p value of 0.01 or less was considered statistically significant.
Results
The overall response rate was 86.4%. Of 851 eligible family physicians, 778 (91.4%) responded. Of the 359 eligible obstetricians 273 (76.0%) responded, and 46 (78.0%) of 59 registered midwives. At the time of the survey, there were no midwives practising in the Northwest region.
Provider characteristics
There were more male than female respondents in all regions except the East (Table 1). There was no regional difference in age, but respondents in urban centres were older than those in rural areas (mean 41.7 v. 39.3 years, p < 0.001). Most of the respondents (39.4%) were practising in the Central East region, which includes Toronto, and more family physicians (31.2%) practised in rural communities than did obstetricians (18.6%) and midwives (8.4%, p = 0.001).
Table 1. Characteristics, use of maternal serum screening (MSS) and access to services of health care providers who responded to a survey on the Ontario MSS Program, * by practice location
Compared with respondents in rural areas, those in urban centres cared for more pregnant women in the previous year (mean 108.0 v. 51.2, p < 0.001), performed more deliveries (mean 158.8 v. 58.5, p < 0.001) and had provided antenatal care longer (mean 12.1 v. 10.4 years, p = 0.002). Respondents in the Central East region performed more deliveries than those in the other regions (mean 155.6 v. 58.3-130.4, p < 0.001), and a larger proportion cared for at least 50 pregnant women in the last year (difference not significant) (Table 1).
Practices regarding MSS
In all but one of the regions, between 84.4% and 91.5% of the respondents stated that they routinely offer MSS to all pregnant women in their practices; in the Northwest region the proportion was only 71.4% (Table 1). MSS was more likely to be offered routinely by respondents in urban centres than by those in rural areas (90.1% v. 81.9%, p = 0.001). Most of the respondents in the Northwest region (53.1%) felt that patient characteristics affect the offering of MSS. These were identified as low education level, cultural differences (including aboriginal heritage), language barriers and low socioeconomic status.
In the Central East region a significantly higher proportion of women under the age of 35 years who were offered MSS chose to have the test than did those in the 2 northern regions (Table 1). Compared with pregnant women in rural areas, those in urban areas under 35 years of age were more likely to choose to have the test (62.9% v. 45.1%, p < 0.001), and those 35 years or more were more likely to have some form of genetic screening (MSS, chorionic villus sampling or amniocentesis) (76.1% v. 62.9%, p < 0.001).
Opinions
Although many of the respondents agreed that too many women with normal pregnancies have positive MSS results (range across regions 42.4%-77.4%), the highest proportion was in the Northwest region (p = 0.001). Compared with respondents in the Central East region, those in the Northwest region were more likely to indicate that the MSS protocol was too complicated (41.9% v. 10.1%, p = 0.001), that the test implications were too complex (53.1% v. 26.9%, p < 0.001) and that there were more important priorities for health care funding (53.3% v. 26.3%, p = 0.001).
Over half (53.1%) of the respondents in the Central East region agreed that educating women about MSS reduced their anxiety, as compared with 26.2% of respondents in the Northeast and 24.1% in the Northwest (p = 0.001). Respondents in the Northwest region were more likely than those in the other regions to disagree that genetic tests to detect fetal abnormalities should be made available to all pregnant women (25.0% v. 9.5%-19.4%, p = 0.001).
Access to services
Fewer respondents in the 2 northern regions than in the other regions agreed that follow-up services (amniocentesis, detailed ultrasound and genetic counselling) and abortion services were readily available in their communities (Table 1). A similar difference was noted between respondents in rural and urban areas regarding the availability of follow-up services (46.3% v. 77.7% respectively, p = 0.001) and abortion services (22.8% v. 51.2% respectively, p = 0.001). Although respondents in all regions reported that positive results were received quickly, it took significantly longer to receive negative results in the northern regions (mean 10.6 days in the Northwest and 10.1 in the Northeast) than in the Central East region (mean 8.4) (p = 0.002).
Recommendations
Respondents in the Central East region (64.6%) were more likely than those in the Northwest region to recommend not changing the MSS program (64.6% v. 7.1%, p = 0.001); more respondents in urban centres than in rural areas also felt this way (52.9% v. 39.8%, p = 0.001). Respondents in the Northwest region were more likely than those in the Central East to recommend discontinuing the program (39.3% v. 12.1%, p = 0.001) and to recommend changing it (53.6% v. 23.3%, p = 0.001). Suggestions for modifying the test included improving the written patient information, making the offering of MSS elective and offering MSS only to selected patients (e.g., those with high-risk pregnancies).
The results of the logistic regression analysis, conducted to determine which variables independently accounted for differences in the routine offering of MSS to all pregnant women, are presented in Table 2. This model controlled for planning region, community (urban or rural), provider age and sex, number of pregnant women cared for in the previous year, whether respondents felt that patient characteristics affect the offering of MSS, attitudes toward MSS (complexity of test and protocol, time involved in counselling) and the availability of follow-up and abortion services. After these factors were controlled for, regional differences disappeared except in the East region, where respondents were less likely to offer MSS routinely than their counterparts in the Central East region (odds ratio [OR] 0.50, 95% confidence interval [CI] 0.27-0.91). Differences between respondents in urban and rural areas who routinely offered MSS also disappeared. The model also showed that respondents who cared for at least 50 pregnant patients in the last year were more likely than those who cared for fewer than 50 to offer MSS routinely (OR 2.00, 95% CI 1.21-3.27). Respondents who felt that patient characteristics affect the offering of MSS (OR 0.42, 95% CI 0.26-0.67) and those who felt that follow-up services were not readily available (OR 0.33, 95% CI 0.20-0.55) were less likely to offer the test routinely than were respondents who felt otherwise.
Table 2. Factors associated with the routine offering of MSS to all pregnant women
Interpretation
The results of our study showed that respondents in northern and rural Ontario were less likely than those in other regions and urban centres to offer MSS routinely to all pregnant women in their practices. Those in the Northwest region were most likely to feel that patient factors affect their offering of this test, and respondents in northern and rural Ontario were most likely to feel that follow-up services were not readily available. In the regression analysis, these were significant factors affecting the routine offering of MSS.
Respondents in the Central East region (includes Toronto) and those in urban centres were most likely to recommend not changing the program. Before the introduction of the MSS program, some pregnant women in Toronto and areas of southern Ontario were being offered screening with single or triple markers. Providers in these areas have had more exposure to and experience using the test, which may have influenced their practice patterns and opinions.
The respondents in the Northwest region were more likely to recommend discontinuing or changing the program and were less likely to offer MSS routinely compared with those in the Central East region. This finding was consistent with their opinions of MSS; they believed that the test's false-positive rate was too high, the protocol too complex and counselling too time consuming and that there were more important funding priorities.
Respondents in the northern regions and those in rural areas expressed concerns about availability of follow-up and abortion services. In a 1997 press release the Institute for Clinical Evaluative Sciences in Ontario revealed that 94% of hospitals in Toronto performed abortions, as compared with only 30% of hospitals in the Northeast region. [15] This highlights the importance of addressing service needs before the introduction of new tests.
Ontario Ministry of Health statistics revealed that in the first 2 years of the MSS program 65% of pregnant women in the Toronto area chose to have the test, as compared with only 25% in northern Ontario. [6] What factors, therefore, influence a woman's decision regarding prenatal genetic screening? Studies of maternal serum alpha-fetoprotein screening have shown that the nature of the information given to women, and how it was presented, influenced whether screening was done. [16, 17]
After we controlled for provider characteristics, we found that practice location was probably not the most important factor in determining the likelihood of routinely offering MSS and providers' attitudes toward the MSS program. Instead, caring for more pregnant women, feeling that patient characteristics affect the offering of MSS and not having ready access to follow-up services were more important factors. Perhaps respondents with a higher volume of patients were observing more true-positive results and, therefore, saw more value in offering MSS. Addressing the social and cultural sensitivity of MSS and the availability of follow-up services could improve the success of this and similar programs.
There were limitations to this study. Family medicine certificants have been found to differ from nonmembers in demographic characteristics, attitudes and practice patterns. [18–21] The sample we used may not have been fully representative of Ontario family physicians or general practioners who provide antenatal care. The samples in the northern regions were relatively small because of the low numbers of providers practising in these areas; however, the response rates in these regions were similar to those in the other regions of Ontario. Finally, all responses to questions about the use of MSS were self-reported.
In conclusion, we found significant regional differences in health care providers' use and opinions of MSS, access to services and recommendations. Providers in the Northwest region of Ontario and those in rural areas were less likely than those in other regions and urban centres to offer MSS routinely and less likely to recommend keeping the program without changes. After controlling for provider characteristics, however, we found that the only significant factors affecting the routine offering of MSS were caring for a higher volume of pregnant women, providers' perceptions that patient characteristics affect the offering of MSS and the availability of follow-up services. Addressing these issues could help to ensure the success of future programs that introduce genetic screening tests.
We thank the Ontario Maternal Serum Screening Steering Committee for its support of this research. We also thank Dr. Warren McIsaac for his input and all of the health care providers who participated in the study.
Funding for the project was provided by the Ontario Ministry of Health.
Competing interests: None declared.
This article has been peer reviewed.
Reprint requests to: Joanne A. Permaul-Woods, Department of Family Medicine, Mount Sinai Hospital, 413-600 University Ave., Toronto ON M5G 1X5; fax 416 586-3175
References
- 1.
- 2.
- 3.
- 4.
- 5.
- 6.
- 7.
- 8.
- 9.
- 10.
- 11.
- 12.
- 13.
- 14.
- 15.
- 16.
- 17.
- 18.
- 19.
- 20.
- 21.