


Abstract
Background: Induction of labour is common, and cesarean delivery is regarded as its major complication. We conducted a systematic review and meta-analysis to investigate whether the risk of cesarean delivery is higher or lower following labour induction compared with expectant management.
Methods: We searched 6 electronic databases for relevant articles published through April 2012 to identify randomized controlled trials (RCTs) in which labour induction was compared with placebo or expectant management among women with a viable singleton pregnancy. We assessed risk of bias and obtained data on rates of cesarean delivery. We used regression analysis techniques to explore the effect of patient characteristics, induction methods and study quality on risk of cesarean delivery.
Results: We identified 157 eligible RCTs (n = 31 085). Overall, the risk of cesarean delivery was 12% lower with labour induction than with expectant management (pooled relative risk [RR] 0.88, 95% confidence interval [CI] 0.84–0.93; I2 = 0%). The effect was significant in term and post-term gestations but not in preterm gestations. Meta-regression analysis showed that initial cervical score, indication for induction and method of induction did not alter the main result. There was a reduced risk of fetal death (RR 0.50, 95% CI 0.25–0.99; I2 = 0%) and admission to a neonatal intensive care unit (RR 0.86, 95% CI 0.79–0.94), and no impact on maternal death (RR 1.00, 95% CI 0.10–9.57; I2 = 0%) with labour induction.
Interpretation: The risk of cesarean delivery was lower among women whose labour was induced than among those managed expectantly in term and post-term gestations. There were benefits for the fetus and no increased risk of maternal death.
Labour is induced in 1 of 5 births1,2 for maternal reasons (e.g., preeclampsia, cardiac or renal disease), fetal reasons (e.g., intrauterine growth restriction) or a combination (e.g., poorly controlled diabetes, preterm rupture of the membranes or post-term pregnancy).3 Induction of labour artificially ripens the cervix and initiates uterine contractions in women who are not already in labour, leading to progressive dilation of the cervix to achieve vaginal birth of a baby at any gestation beyond the legal definition of fetal viability.4
Although induction of labour has been criticized for an associated increased risk of cesarean delivery, recent studies have shown that there are fewer cesarean deliveries with induction than without it. However, the findings have not had much impact on practice, in part because the systematic reviews5–8 investigated subsets of induction and included few randomized controlled trials (RCTs), and because observational data in a cohort study9 had risk of confounding. Consumer organizations,10 guidelines11 and textbooks12,13 have given contradictory information about cesarean risk, which can lead to confusion over decision-making, particularly given a desire to support normal birth in the face of increasing cesarean rates worldwide. Cesarean delivery carries multiple risks to mother and baby, including maternal death,14 infection and postnatal depression,15,16 and respiratory distress syndrome in neonates.14 Accurate, precise information about cesarean risk is therefore needed for decision-making regarding labour induction.
We conducted a systematic review and meta-analysis of RCTs to investigate the risk of cesarean delivery associated with labour induction compared with expectant management. We also explored the effects of clinical characteristics and study quality on the overall result using subgroup and meta-regression analyses.
Methods
Data sources and study selection
In April 2012, we searched the electronic databases MEDLINE, Embase, CAB Abstracts, CENTRAL (the Cochrane Central Register of Controlled Trials) and Science Citation Index (accessed via Web of Science) for eligible RCTs using the search terms and word variants for the concept “labour induction” and “cesarean delivery.” The search strategy is outlined in Appendix 1 (available at www.cmaj.ca/lookup/suppl/doi:10.1503/cmaj.130925/-/DC1). The Cochrane Database of Systematic Reviews was also searched for primary trials. Titles and abstracts of all citations were assessed for inclusion by 2 of 3 reviewers (C.M., E.R. or E.M.). Disagreements were resolved through consensus with input from the third reviewer.
We included RCTs if they recruited pregnant women carrying a viable fetus, they compared an active induction with placebo or expectant management (hereafter referred to as expectant management), and they reported rates of cesarean delivery as one of the outcomes. Methods of active intervention included mechanical methods (amniotomy, membrane sweeping, Foley catheter insertion with or without extra-amniotic saline infusion), use of pharmacologic agents (prostaglandins, oxytocin, corticosteroids, mifepristone, estrogens, relaxin, misoprostol, isosorbide mononitrate) and alternative methods (acupuncture, breast stimulation, sexual intercourse, homeopathic preparations, castor oil, bath, enema). We excluded RCTs that recruited women who had a multiple pregnancy or were in active labour, those in which an active intervention was applied in the control group or within 12 hours after randomization and trials in which the control group comprised women in spontaneous labour. No restrictions were applied to year, language or publication status.
Data extraction and quality assessment
Two of us (E.R. and E.M.) independently extracted the following data from the trials: method of induction, reason for induction, and number of cesarean and noncesarean (vaginal or instrumental) deliveries in the intervention and control groups, and information required to assess methodologic quality. Many of the efficacy or safety studies did not provide reasons for labour induction. If primary trials were inaccessible through online and library databases, we extracted information from the Cochrane Database of Systematic Reviews and contacted the authors of the trial to confirm the results.
For the assessment of methodologic quality, we evaluated the following parameters for risk of bias: sequence generation, allocation concealment, blinding of participants and personnel, and management of incomplete output data.17 We did not assess blinding of participants and personnel in trials that used mechanical interventions because it cannot be applied in such situations.
Disagreements in grouping, coding or quality assessment were resolved through consensus with input from a third author (C.M. or K.S.K.).
Data synthesis
We assessed heterogeneity between trials by inspecting forest plots and using the I2 statistic (I2 values of 25%, 50% and 75% corresponded to cut-off points of low, moderate and high degrees of heterogeneity, respectively).18 For the primary and subgroup analyses, we calculated pooled relative risk (RR) estimates and 95% confidence intervals (CIs) using random-effects models, with each study weighted according to inverse of variance. In a number of trials, some participants were lost to follow-up or were excluded from analyses for other reasons; we therefore used intention-to-treat denominators in the meta-analyses. In the subgroup meta-analyses, we investigated whether risk of cesarean delivery differed according to indication for labour induction, induction method, gestational age (term, preterm or post-term), definition of induction (cervical priming, induction of uterine contractions or both), cervical status (unfavourable or favourable), pregnancy risk (high or low) and parity (nulliparous or parous).
We used meta-regression analysis to explore whether patient characteristics (indication for induction, gestational age at induction, cervical score, pregnancy risk, parity), induction methods (type of intervention and definition of induction [cervical priming v. no cervical priming]) and study quality (random sequence generation, allocation concealment, performance bias and attrition bias) explained the heterogeneity. We also evaluated safety (in terms of maternal and fetal deaths, and admission to neonatal intensive care unit) and methods of induction currently used in clinical practice in the United Kingdom, Canada and the United States.1,2,19 We used the Harbord modified test for small-study effects to examine publication bias in funnel plots.
We used Review Manager software (RevMan version 5.2; Nordic Cochrane Centre, Cochrane Collaboration, 2012) to conduct the meta-analyses and Stata software (Stata Statistical Software, release 11; StataCorp; 2009) to perform the meta-regression analyses.
Results
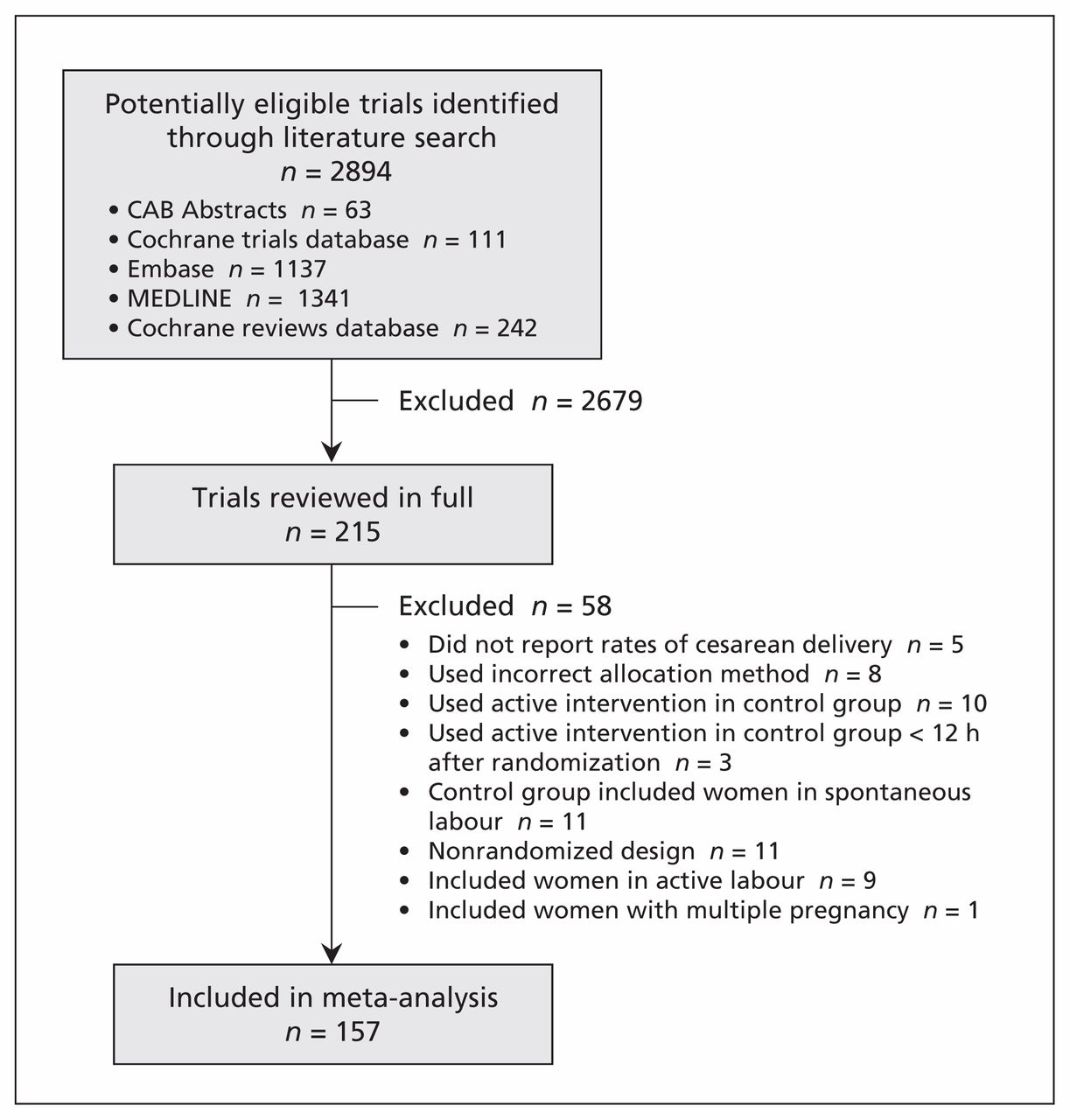
We identified 2894 potentially relevant studies through the literature search. The selection of trials for our meta-analysis is summarized in Figure 1. After the screening of titles and abstracts and removal of duplicate records, 215 articles were reviewed in full. We excluded 58 because they did not report rates of cesarean delivery (5 trials), the active intervention was applied in the control group (10) or within 12 hours after randomization (3), an incorrect allocation method was used (8), the control group included women in spontaneous labour (11), the study had a nonrandomized design (11), women in active labour were included at the time of randomization (9), or the trial included women with a multiple pregnancy (1). The excluded studies, with reason for exclusion, are listed in Appendix 2 (available at www.cmaj.ca/lookup/suppl/doi:10.1503/cmaj.130925/-/DC1).
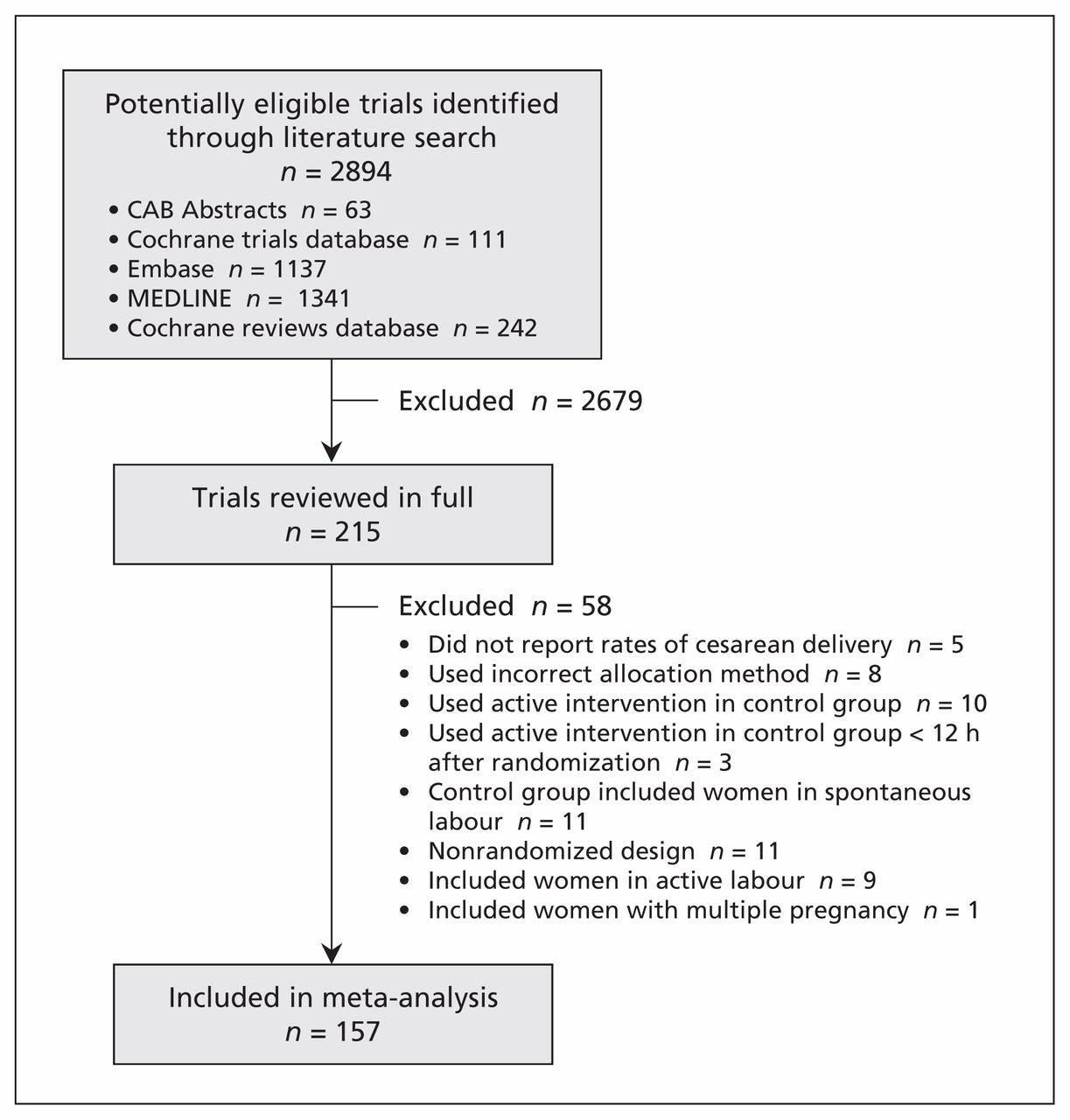
Selection of randomized controlled trials for the meta-analysis.
Characteristics of the 157 RCTs (n = 31 085) included in the meta-analysis20–176 are summarized in Appendix 3 (available at www.cmaj.ca/lookup/suppl/doi:10.1503/cmaj.130925/-/DC1). Despite extensive searches, we were unable to retrieve the reports of 4 trials; we extracted available clinical results for the trials from the Cochrane Database of Systematic Reviews107,124,125,146 but did not have access to data about the study design to assess their methodologic quality. The results of the quality assessment for the other RCTs are summarized in Figure 2 and shown for each trial in Appendix 4 (available at www.cmaj.ca/lookup/suppl/doi:10.1503/cmaj.130925/-/DC1).

Risk-of-bias assessment of trials included in the meta-analysis. Results for individual trials are shown in Appendix 4 (available at www.cmaj.ca/lookup/suppl/doi:10.1503/cmaj.130925/-/DC1).
The summary results of the primary and subgroup meta-analyses are shown in Figure 3. Results for the individual trials are shown in Appendix 5 (available at www.cmaj.ca/lookup/suppl/doi:10.1503/cmaj.130925/-/DC1). Overall, the risk of cesarean delivery was lower with labour induction than with expectant management (pooled RR 0.88, 95% CI 0.84–0.93). Statistical heterogeneity was low (I2 = 0%). Nevertheless, planned meta-regression analysis to explain heterogeneity did not show a significant impact of variables on the main result (Appendix 6, available at www.cmaj.ca/lookup/suppl/doi:10.1503/cmaj.130925/-/DC1). In particular, initial cervical score (p = 0.4), indication for induction (p = 0.8) and method of induction (p = 0.6) did not alter the main result. The test for publication bias was not significant (p = 0.5) (Appendix 7, available at www.cmaj.ca/lookup/suppl/doi:10.1503/cmaj.130925/-/DC1).

Overall and subgroup analyses investigating the effect of induction of labour versus expectant management on the risk of cesarean delivery. Values less than 1 indicate a decreased risk of cesarean delivery. *Acupuncture, breast stimulation, sexual intercourse, homeopathic preparations, castor oil, bath or enema. †Gestation > 40 wk. CI = confidence interval.
In the subgroup analysis by method of induction (Figure 3), 4 methods were associated with a significant reduction in risk of cesarean delivery: prostaglandin E2 (RR 0.90, 95% CI 0.84–0.96; I2 = 0%), misoprostol (RR 0.62, 95% CI 0.48–0.81; I2 = 0%), alternative method (RR 0.66, 95% CI 0.50–0.86; I2 = 60.7%) and mixed method (RR 0.81, 95% CI 0.70–0.95; I2 = 0%). Subgroup analysis by indication for induction showed a universal reduction in risk of cesarean delivery. Induction without a medical indication provided was associated with risk reduction of 19% (RR 0.81, 95% CI 0.70–0.93; I2 = 13.5%). When we looked at risk of cesarean delivery by gestational age, we found statistically significant reductions in risk with labour induction in term and post-term pregnancies, but not in preterm pregnancies. In the analysis by definition of induction, risk of cesarean delivery was significantly lower when the definition included cervical ripening alone or combined with stimulation of uterine contractions than when it included uterine stimulation alone. The analysis by cervical status showed a 13% reduction in risk of cesarean delivery if the cervix was unfavourable at induction (RR 0.87, 95% CI 0.81–0.94; I2 = 1.4%) and no difference in risk if the cervix was favourable (RR 0.83, 95% CI 0.60–1.14; I2 = 0%). The risk of cesarean delivery was reduced in both high- and low-risk pregnancies.
Results from studies with low risk of bias related to allocation concealment were compatible with the main finding (RR 0.89, 95% CI 0.80–0.99, I2 = 9%). Exclusion of induction methods not currently used in clinical practice in the UK, Canada and the US (relaxin, isosorbide mononitrate, mifepristone, corticosteroids and alternative methods described earlier in the methods) showed an effect comparable to the main result (RR 0.89, 95% CI 0.84–0.93; I2 = 0%).
Analysis of adverse outcomes showed a lower risk of fetal death and admission to neonatal intensive care unit associated with labour induction than with expectant management (Table 1). No impact on maternal death was shown.
Risk of adverse outcomes associated with labour induction versus expectant management
Interpretation
Our meta-analysis showed that the risk of cesarean delivery following labour induction was significantly lower than the risk associated with expectant management. This finding supports evidence from systematic reviews5–8 but is contrary to prevalent beliefs and information from consumer organizations, guidelines and textbooks.10–13 Labour induction was associated with benefits for the fetus and no increased risk of maternal death.
Subgroup analysis by method of induction showed a significant reduction in risk of cesarean delivery associated with the use of prostaglandin E analogues (prostaglandin E2 and misoprostol). This is encouraging, since use of prostaglandin E2 is the main method of induction in the UK and the main method of cervical ripening in the US and Canada.1,2,19 However, use of oxytocin and amniotomy, still widely practised induction methods, did not confer a benefit on cesarean delivery. In the subgroup analysis by indication for induction, mixed reason (maternal, fetal and obstetric) and post-dates pregnancy were associated with a reduced risk of cesarean delivery. In uncomplicated term pregnancies with no medical reason for induction provided, the risk of cesarean delivery was reduced by 19% on average. We also observed risk reductions associated with induction in term and post-term pregnancies and in high- and low-risk pregnancies. Our findings are important when selecting candidates for labour induction and when advising women on the risks of induction.
Limitations
Our study has limitations. We could not retrieve and verify 4 primary studies and therefore had to use numeric data obtained from the Cochrane Database of Systematic Reviews. However, the reliance on these data likely did not have much effect on the results because our analysis including the remaining 153 studies was sufficiently powerful for reliable inferences. When we updated our searches in February 2014, we found 336 new citations published since April 2012. Of these, only 2 trials177,178 met our inclusion criteria. The number of participants in the trials was 636, which represented 2% of the total in our current analysis. Both studies concluded that there was no effect on cesarean delivery rates with relative imprecision, so our main conclusion remains robust.
We restricted our analyses to RCTs with appropriate sequence generation, minimizing the risk of bias and confounding. Concealment of allocation was reported unclearly in half of the studies, risking bias in both the clinical management of the women and the assessment of outcomes. However, studies with a low risk of bias in allocation concealment supported the main finding.
We explored many potential confounding factors but did not account for all. For example, body mass index and maternal age may be associated with increased rates of complication. We could not always disentangle reasons for induction and had to lump together maternal, fetal and obstetric indications, leading to some difficulty in interpretation.
We included studies dating from 1975 to 2010; therefore, differences in practice over this time period may have influenced the findings. These issues would be best addressed in a meta-analysis of individual patient data.
Although 2 of us abstracted the study data independently, errors in coding may have occurred and thus are a potential source of bias. This is especially true for the definition of induction and assessment of pregnancy risk, because these parameters were not always defined in detail in the primary studies and had to be judged.
Conclusion
Our meta-analysis has provided a robust answer to the disputed question of risk of cesarean delivery associated with induction of labour. Women whose labour was induced were less likely than those managed expectantly to have a cesarean delivery. In addition, the risk of fetal death and admission to neonatal intensive care unit were decreased in the induction group. Our findings have implications for guidelines and the practice of obstetrics, and are reassuring for mothers, midwifes and obstetricians.
Footnotes
Competing interests: None declared.
This article has been peer reviewed.
Contributors: Ekaterina Mishanina conducted the Cochrane database searches, made inclusion and exclusion decisions, extracted data, performed methodologic quality assessment and wrote some of the manuscript. Ewelina Rogozinska conducted the literature search, extracted data, performed methodologic quality assessment, contributed to the analysis and contributed to the writing of the manuscript. Tej Thatthi helped with this project as part of his placement from a medical school in Kenya. He obtained journal articles, helped with inclusion and exclusion decisions and contributed to the writing of the manuscript. Rehan Uddin-Khan contributed to the interpretation of data and to the writing of the manuscript. Khalid Khan conceived the idea of the meta-analysis, provided the overall direction of the project, conducted the meta-regression analysis and revised the manuscript. Catherine Meads supervised Ekaterina Mishanina, Ewelina Rogozinska and Tej Thatthi, conducted data extraction and contributed to the writing of the manuscript. All of the authors approved the final version of the manuscript submitted for publication and agreed to act as guarantors of the work.
References
In this issue

{kind=link}
{kind=link}
{kind=link}
Article tools






Jump to section
Related Articles
Cited By...
- The Long-Run Effects of Cesarean Sections
- Breaking the myth: the association between the increasing incidence of labour induction and the rate of caesarean delivery in Finland - a nationwide Medical Birth Register study
- Fetal movement awareness raising: more harm than good!
- Timing of delivery in women with pre-pregnancy diabetes mellitus: a population-based study
- Fetal movement awareness raising: more harm than good!
- Healthy Birth Practice #1: Let Labor Begin on Its Own
- Preventing venous thromboembolism during pregnancy and postpartum: crossing the threshold
- Caesarean sections and private insurance: systematic review and meta-analysis
- Caesarean sections and for-profit status of hospitals: systematic review and meta-analysis
- Induction of labour decreases a woman's chance of caesarean delivery when compared with expectant management
- Induction of labour
- Induction of labour
- Induction of labour
More in this TOC Section
Similar Articles
Collections

