


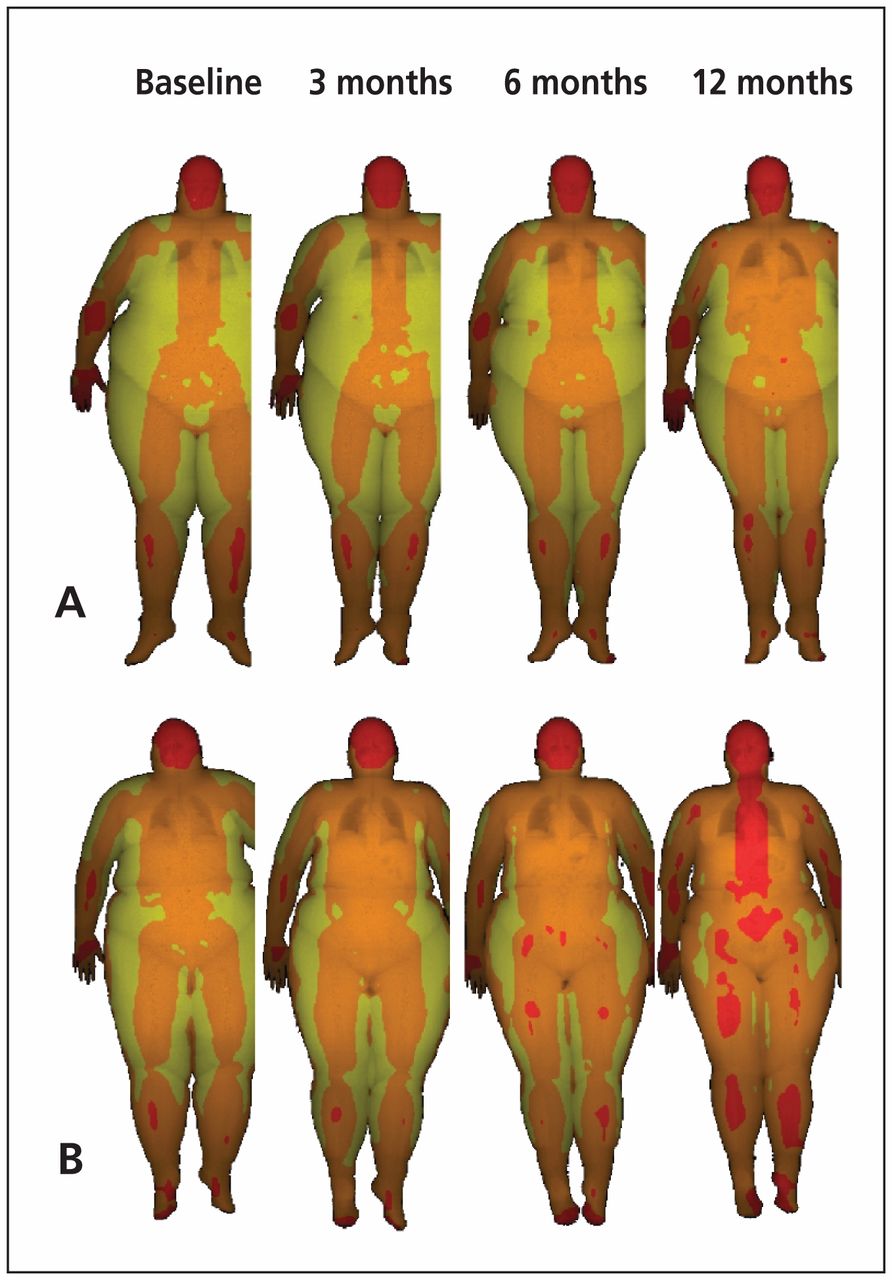
Two patients with grade III obesity (body mass index [BMI] ≥ 40), a 31-year-old man (A) and a 26-year-old woman (B), banded gastroplasty. Both patients followed the same nutritional and postsurgical approach. After 12 months, both patients achieved a similar reduction in BMI (patient A: −29.7%; patient B: −28.8%) and other relevant anthropometric measures (e.g., waist circumference, waist-to-hip ratio). However, changes in body mass composition differed between the 2 patients (Figure 1, Appendix 1 [available at www.cmaj.ca/lookup/suppl/doi:10.1503/cmaj.120149/-/DC1]). Dual-energy x-ray absorptiometry (DXA) analysis showed opposite trends in their fat and lean compartments (Figure 1): patient B had higher percentage decreases in total (patient B: −30.2%; patient A: −12.2%) and android or central (patient B: −34.0%; patient A: −14.7%) fat. Patient B had a greater loss of visceral fat mass in the android region (patient B: 2700 g to 471 g [−82.6%]; patient A: 4191 g to 2439 g [−41.8%]).
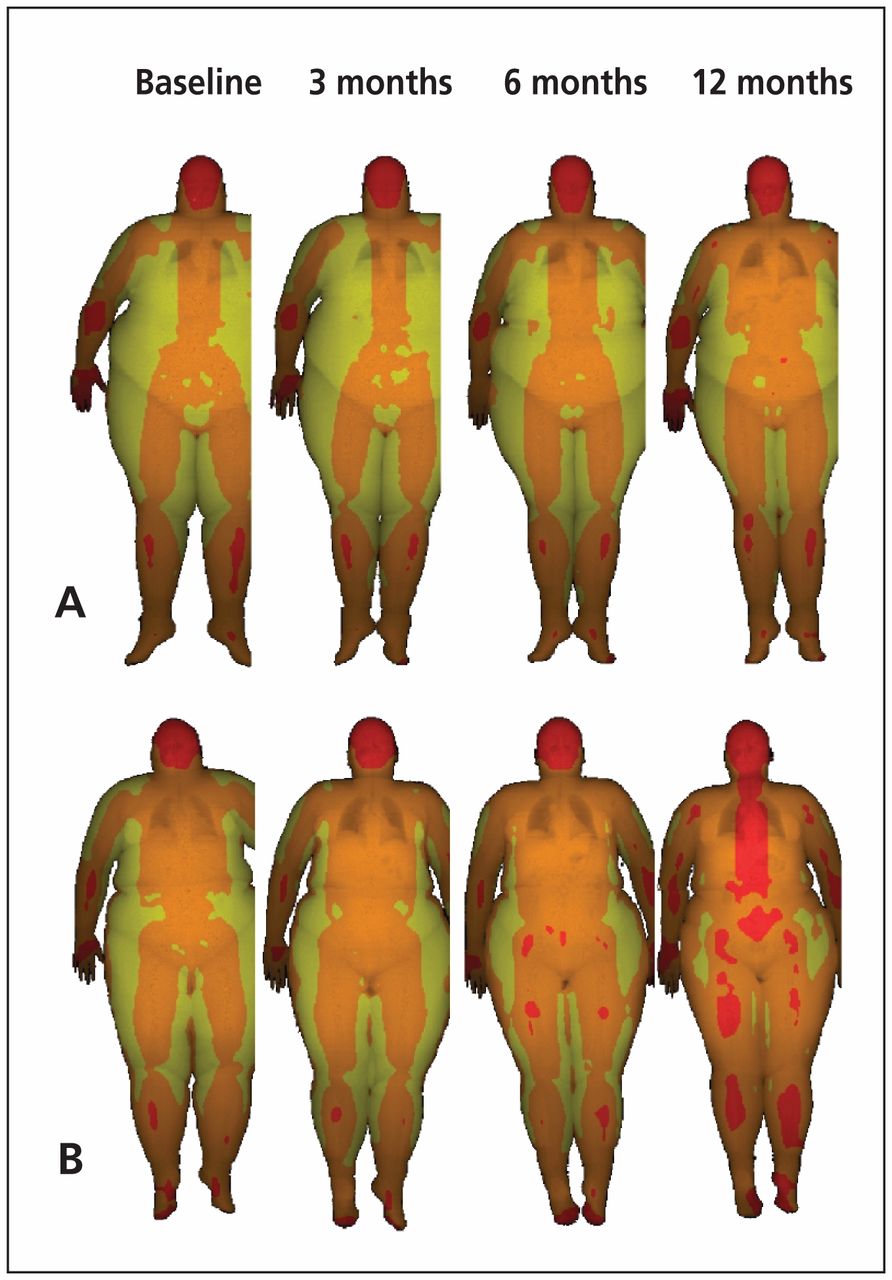
Dual-energy x-ray absorptiometry performed after bariatric surgery in a 31-year-old man (patient A) and a 26-year-old woman (patient B) with grade III obesity. Body composition is indicated by colour: red < 25% fat; orange 25%–60% fat; and yellow ≥ 60% fat. For more information on this technique, see Appendix 1.
Obesity is caused by a complex interaction of environmental factors, human behaviour and genetic predisposition, and it is associated with high mortality and risk of various chronic diseases.1 The distribution of adiposity has more influence on outcomes than the total amount of body fat; in particular, an android pattern of fat mass is associated with an increased risk of metabolism-related disorders.2 The location of fat (visceral or subcutaneous) also has different effects on the development and pathogenesis of metabolic and cardiovascular diseases, with increased visceral fat being associated with an adverse metabolic profile.2
Body mass index and other common anthropometric measures do not accurately flect body composition and compartmental distribution of fat mass.3 Hence, we used DXA for patients A and B to determine body composition and risk of metabolic, cardiovascular and other related diseases.4,5 Despite having similar BMI and anthropometric measures, their body fat distribution in response to surgical treatment and nutritional and rehabilitation protocols after surgery was very different, which may affect their long-term outcomes.
Footnotes
-
Competing interests: None declared.
-
This article has been peer reviewed.
In this issue

{kind=link}
Article tools






Related Articles
Cited By...
- No citing articles found.
More in this TOC Section
Similar Articles
Collections

