


Article Figures & Tables
Figures
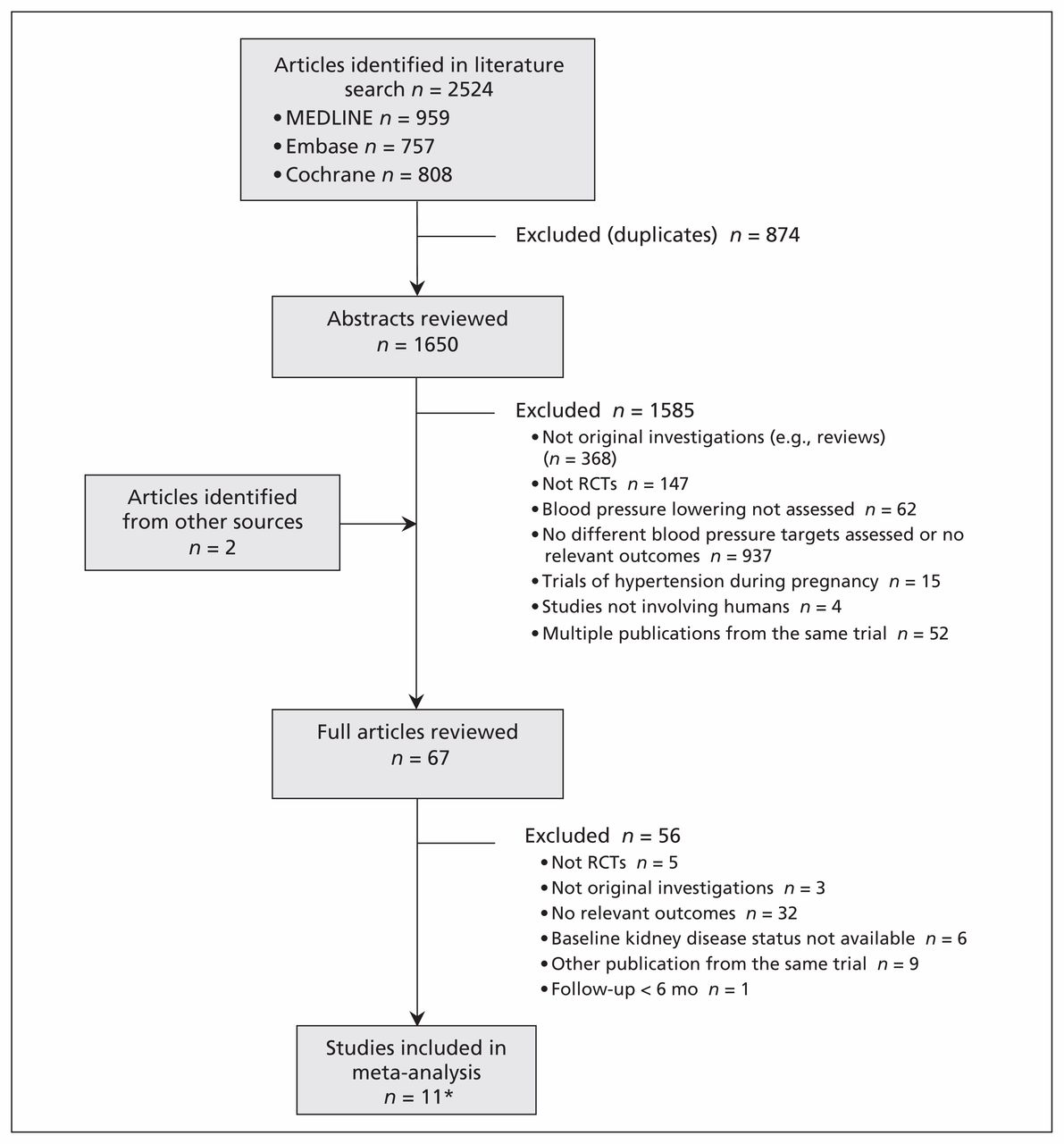
- Figure 1:
Identification of relevant studies for inclusion in the meta-analysis. RCT = randomized controlled trial. *Included studies were published in 12 articles.
- Figure 2:
Effects of intensive blood pressure lowering on progressive kidney failure. BP = blood pressure, CI = confidence interval, ESKD = end-stage kidney disease, HR = hazard ratio. Note: Weights are from random effects analysis.
- Figure 3:
Subgroup analysis of the effect of intensive blood pressure lowering on kidney failure in patients with proteinuria compared with those without proteinuria. CI = confidence interval, HR = hazard ratio.



Tables
Study Inclusion criteria BP, mm Hg Regimen used to achieve target BP Follow-up, yr Patient characteristic Baseline, systolic/diastolic Target in intervention group Target in control group Total, no. With CKD, no. Age, mean, yr Female sex, % Diabetes mellitus, % Kidney failure, no. Major CV event, no. Studies that only recruited patients with CKD AASK (Appel et al. (13); Wright et al. (26)) African American, hypertension, GFR 20–65 mL/min per 1.73 m2 and no other identified causes of renal insufficiency 150.5/95.5 Mean < 92 Mean 102–107 3 × 2 study design; participants were separately and randomly assigned to a class of drugs (ramipril, metoprolol or amlodipine) and separately to the BP target; in the cohort phase, all were switched from randomized therapy to ramipril 8.8–12.2 1 094 1 094 55 38.8 Excluded 422¶ 225 Ruggenenti et al. (14) Nondiabetic nephropathy with proteinuria 1–3 g/d and GFR < 45 mL/min per 1.73 m2 or proteinuria > 3 g/d and GFR < 70 mL/min per 1.73 m2 136.7/84.1 < 130/80 Diastolic < 90 All patients were given ramipril and received add-on therapy with felodipine as required 1.6 338 338 54 25.7 Excluded 72‡ 9 Klahr et al. (17) CKD, serum creatinine 1.4–7.0 mg/dL (male) or 1.2–7.0 mg/dL (female) 130.5/80 Mean < 92 Mean < 107 ACE inhibitors, with or without a diuretic 16.7 840 840 52 40 5.10 616‡ NR* Wühl et al. (18) CKD, age 3–18 yr and GFR 15–80 mL/min per 1.73 m2 with 24-h mean BP elevated or controlled by antihypertensive agents 118.3/73.0 24-hr mean BP < 50th percentile 24-hr mean BP in the 50th– 95th percentile All patients were given ramipril and received any other class of antihypertensive agents as required 5.0 385 385 12 41 NR† 115§ NR Toto et al. (21) Hypertensive nephrosclerosis, serum creatinine > 1.6 mg/dL or GFR < 70 mL/min per 1.73 m2 123.1/76.5 Diastolic, 65– 80 Diastolic, 85– 95 2 × 2 study design; patients were randomized to either placebo or enalapril and then a stepped-care approach: diuretic; n-blocker; hydralazineor minoxidil; and clonidine, α-methyldopa or R1- blocker 3.4 77 77 56 37.7 Excluded 19† NR Schrier et al. (28) Autosomal-dominant polycystic kidney disease with hypertension and left ventricular hypertrophy; age 20–60 yr; creatinine clearance > 30 mL/min; 142.5/94.5 < 120/80 < 135–140/85–90 Patients were randomized to either enalapril- or amlodipine-based approaches 7.0 75 75 41 45 NR 8‡ NR Studies reporting subgroup data for patients with CKD UK Prospective Diabetes Study Group (22)* Newly diagnosed type 2 diabetes mellitus with hypertension 159.3/94 < 150/85 < 180/105 Captopril or atenolol 8.4 1 148 103 56 44.5 100 NR* NR* Hansson et al. (23)* Hypertension, diastolic BP 100–115 mm Hg 169.7/105.4 Diastolic < 80 Diastolic < 85 or < 90 All initially received felodipine and add-on therapy with ACE inhibitors or β-blockers and then a diuretic 3.8 1 8790 3 619 62 47 8 NR* 186 Estacio et al. (24)* Type 2 diabetes mellitus with diastolic BP ≥ 90 mm Hg 155/98 Diastolic < 75 Diastolic 80–89 Patients were randomized to either enalapril or amlodipine initially, and received add-on with metoprolol and hydrochlorothiazide 5.0 470 120 58 32.6 100 NR* 29 Schrier et al. (25)* Type 2 diabetes mellitus with normotension (diastolic BP 80– 89 mm Hg) 136.4/84.4 Reduction in diastolic BP of 10 mm Hg from baseline Diastolic 80–89 In the intensive group, patients were randomized to either tonisoldipine or enalapril 5.3 480 137 59 45.5 100 NR* 23 Hayashi et al. (27)* Older adults (65–85 yr), hypertension and systolic BP > 160 mm Hg 163/89.6 Systolic < 140 Systolic < 160 All patients received efonidipine and other agents were added as needed 2.0 4 418 2 499 74 64 11.9 13¶ NR Note: ACE = angiotensin-converting enzyme, BP = blood pressure, CKD = chronic kidney disease, CV = cardiovascular, GFR = glomerular filtration rate, NR = not reported.
↵* CKD was determined by estimated GFR < 60 mL/min per 1.73 m2.
↵† Kidney failure defined as either a composite of 50% decline in GFR, 100% increase in serum creatinine or end-stage kidney disease.
↵‡ Kidney failure defined as end-stage kidney disease.
↵§ Kidney failure defined as a composite of 50% decline in GFR or end-stage kidney disease.
↵¶ Kidney failure defined as a composite of 100% increase in serum creatinine or end-stage kidney disease.
In this issue

{kind=link}
{kind=link}
{kind=link}
Article tools






Jump to section
Related Articles
Cited By...
- Quality of systematic reviews supporting the 2017 ACC/AHA and 2018 ESC/ESH guidelines for the management of hypertension
- Thinking Outside the Box: Novel Kidney Protective Strategies in Kidney Transplantation
- Impact of point-of-care screening for hypertension, diabetes and progression of chronic kidney disease in rural Manitoba Indigenous communities
- Effect of intensive blood pressure on the progression of non-diabetic chronic kidney disease at varying degrees of proteinuria
- Intensive Blood Pressure Lowering Should Be the Goal for Most Individuals at High Risk of Cardiovascular Disease Irrespective of Albuminuria
- Effects of Intensive Blood Pressure Control in Patients with and without Albuminuria: Post Hoc Analyses from SPRINT
- Progress in using the electronic health record to improve primary care
- Chronic kidney disease in adults: assessment and management
- Effects of antihypertensives, lipid-modifying drugs, glycaemic control drugs and sodium bicarbonate on the progression of stages 3 and 4 chronic kidney disease in adults: a systematic review and meta-analysis
- 2019 ACC/AHA Guideline on the Primary Prevention of Cardiovascular Disease: Executive Summary: A Report of the American College of Cardiology/American Heart Association Task Force on Clinical Practice Guidelines
- 2019 ACC/AHA Guideline on the Primary Prevention of Cardiovascular Disease: A Report of the American College of Cardiology/American Heart Association Task Force on Clinical Practice Guidelines
- Improving coding and primary care management for patients with chronic kidney disease: an observational controlled study in East London
- Intensive Blood Pressure Targets and Kidney Disease
- Hypertension Management in Diabetes: 2018 Update
- The National CKD Audit: a primary care condition that deserves more attention
- 2017 ACC/AHA/AAPA/ABC/ACPM/AGS/APhA/ASH/ASPC/NMA/PCNA Guideline for the Prevention, Detection, Evaluation, and Management of High Blood Pressure in Adults: A Report of the American College of Cardiology/American Heart Association Task Force on Clinical Practice Guidelines
- 2017 ACC/AHA/AAPA/ABC/ACPM/AGS/APhA/ASH/ASPC/NMA/PCNA Guideline for the Prevention, Detection, Evaluation, and Management of High Blood Pressure in Adults: Executive Summary: A Report of the American College of Cardiology/American Heart Association Task Force on Clinical Practice Guidelines
- 2017 ACC/AHA/AAPA/ABC/ACPM/AGS/APhA/ASH/ASPC/NMA/PCNA Guideline for the Prevention, Detection, Evaluation, and Management of High Blood Pressure in Adults: Executive Summary: A Report of the American College of Cardiology/American Heart Association Task Force on Clinical Practice Guidelines
- 2017 ACC/AHA/AAPA/ABC/ACPM/AGS/APhA/ASH/ASPC/NMA/PCNA Guideline for the Prevention, Detection, Evaluation, and Management of High Blood Pressure in Adults: A Report of the American College of Cardiology/American Heart Association Task Force on Clinical Practice Guidelines
- Effects of Intensive BP Control in CKD
- 2017 ACC/AHA/HFSA Focused Update of the 2013 ACCF/AHA Guideline for the Management of Heart Failure: A Report of the American College of Cardiology/American Heart Association Task Force on Clinical Practice Guidelines and the Heart Failure Society of America
- 2017 ACC/AHA/HFSA Focused Update of the 2013 ACCF/AHA Guideline for the Management of Heart Failure: A Report of the American College of Cardiology/American Heart Association Task Force on Clinical Practice Guidelines and the Heart Failure Society of America
- Time-Varying Association of Individual BP Components with eGFR in Late-Stage CKD
- Etude SPRINT : Donnees probantes sur les cibles precises de la tension arterielle
- SPRINT to evidence for specific blood pressure targets
- Results and lessons from the Spironolactone To Prevent Cardiovascular Events in Early Stage Chronic Kidney Disease (STOP-CKD) randomised controlled trial
- Treating hypertension in patients with medical comorbidities
- Assessing the Validity of Surrogate Outcomes for ESRD: A Meta-Analysis
- Modification of the Relationship Between Blood Pressure and Renal Albumin Permeability by Impaired Excretory Function and Diabetes
- Blood Pressure and Risk of All-Cause Mortality in Advanced Chronic Kidney Disease and Hemodialysis: The Chronic Renal Insufficiency Cohort Study
- Blood pressure targets in chronic kidney disease: Does proteinuria dictate how low we go?
More in this TOC Section
Similar Articles

