


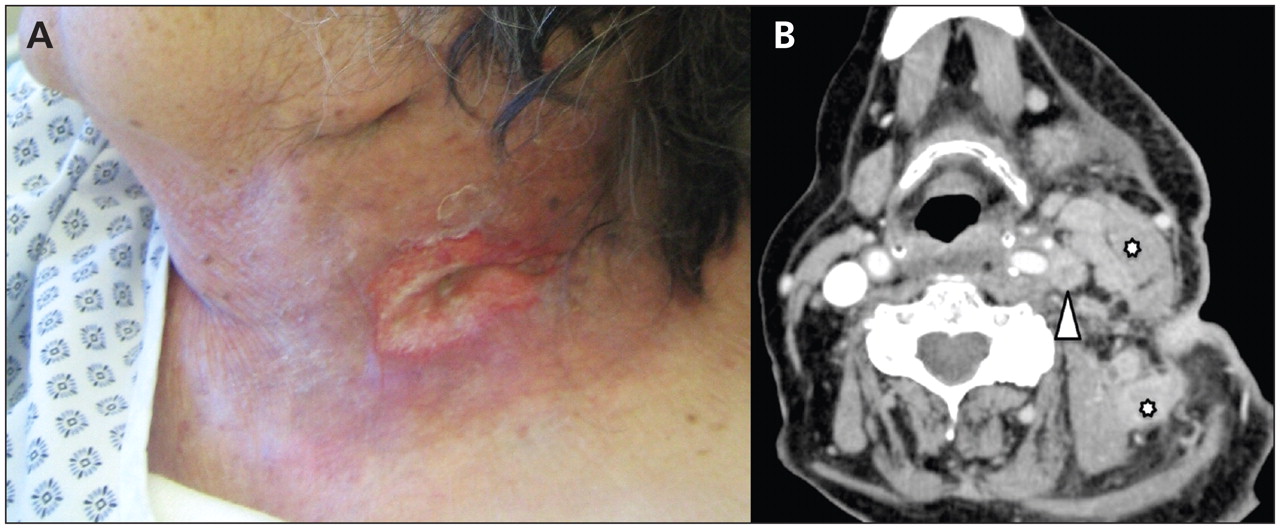
A previously well 77-year-old woman was admitted to hospital with a six-month history of weight loss, fatigue and low-grade fever, and a painless ulcerated mass on her neck.
On examination, the patient had isolated left cervical lymphadenopathy with a draining sinus (Figure 1A). A computed tomography scan showed necrotic inflammation of multiple cervical lymph nodes and a thrombosis of the left internal jugular vein (Figure 1B), in addition to a 30-mm posterior pleural calcification, suggesting tuberculosis sequelae. Direct microscopy of the fluid in the sinus showed acid-fast bacilli. Cultures of the fluid and the patient’s sputum grew Mycobacterium tuberculosis sensitive to first-line antituberculous drugs. No cause of immunosuppression was found (e.g., results of a serological test for HIV were negative).

(A) Ulcerated mass on the neck of a 77-year-old woman. (B) A computed tomography scan shows necrotic inflammation of the patient’s cervical lymph nodes (asterisks) and a thrombosis of her left internal jugular vein (arrowhead).
We prescribed rifampin and isoniazid for nine months, in combination with pyrazinamide and ethambutol for the first two months of the regimen. Prednisone and warfarin were given for the first month until the jugular thrombosis was resolved. Our patient’s condition improved and the sinus was cicatrized on day 40. One year later, our patient has remained well. Her social contacts did not receive treatment because their test results for active or latent infection were negative.
Tuberculous lymphadenitis (scrofula) was known as the “king’s evil” in Europe, where the royal touch was believed to cure the disease until the 18th century.1 Cervical lymphadenitis is the most common presentation of extrapulmonary tuberculosis. Systemic symptoms are often absent in immunocompetent patients; concomitant pulmonary tuberculosis occurs in fewer than 50% of cases.2 Diagnosis is usually by fine-needle aspiration, although excisional biopsy has the highest sensitivity. Results of nucleic acid amplification tests are not reliable.3
The Infectious Diseases Society of America recommends a six-month course of antibiotics. Although treatment with corticosteroids is controversial,2 we used prednisone to alleviate our patient’s venous compression and to prevent a paradoxical upgrading reaction; that is, the worsening of previous lesions, or the appearance of new lesions, after initial improvement.4 This reaction may develop because of a robust immune response to the mycobacterial antigens released with the start of antibiotics.2
Footnotes
-
Competing interests: None declared.
-
This article has been peer reviewed.
In this issue
{kind=link}
Article tools






Jump to section
Related Articles
Cited By...
More in this TOC Section
Similar Articles
Collections

