

An 85-year-old man with a history of stroke presented with a three-day history of bloody stool. He had chronic constipation treated with herbal medicine, but the constipation had become worse over the past two months. On physical examination, there was marked tenderness of the lower abdomen and right hemiparesis. The patient’s hemoglobin level was reduced at 6.39 g/L. A plain abdominal radiograph showed large amounts of feces in the colon and rectum. Computed tomographic scans of the abdomen showed thickening of the rectal wall (Figure 1) and feces in the colon and rectum.
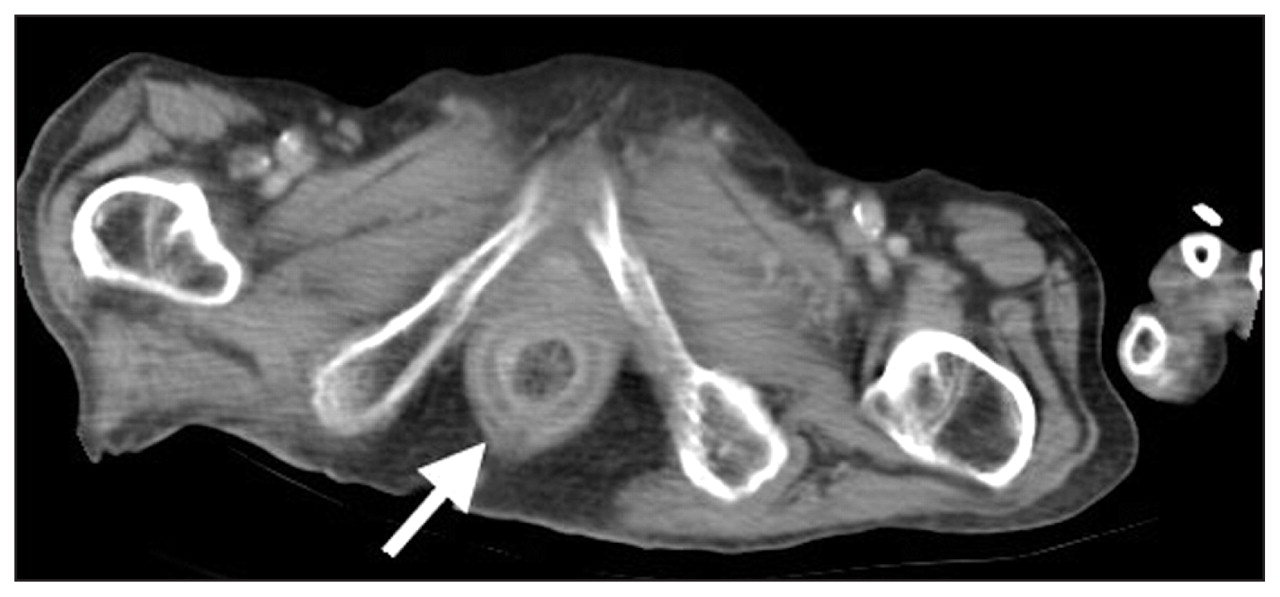
Computed tomographic scan of the abdomen of a man with bloody stool showing a thickened rectal wall (arrow).
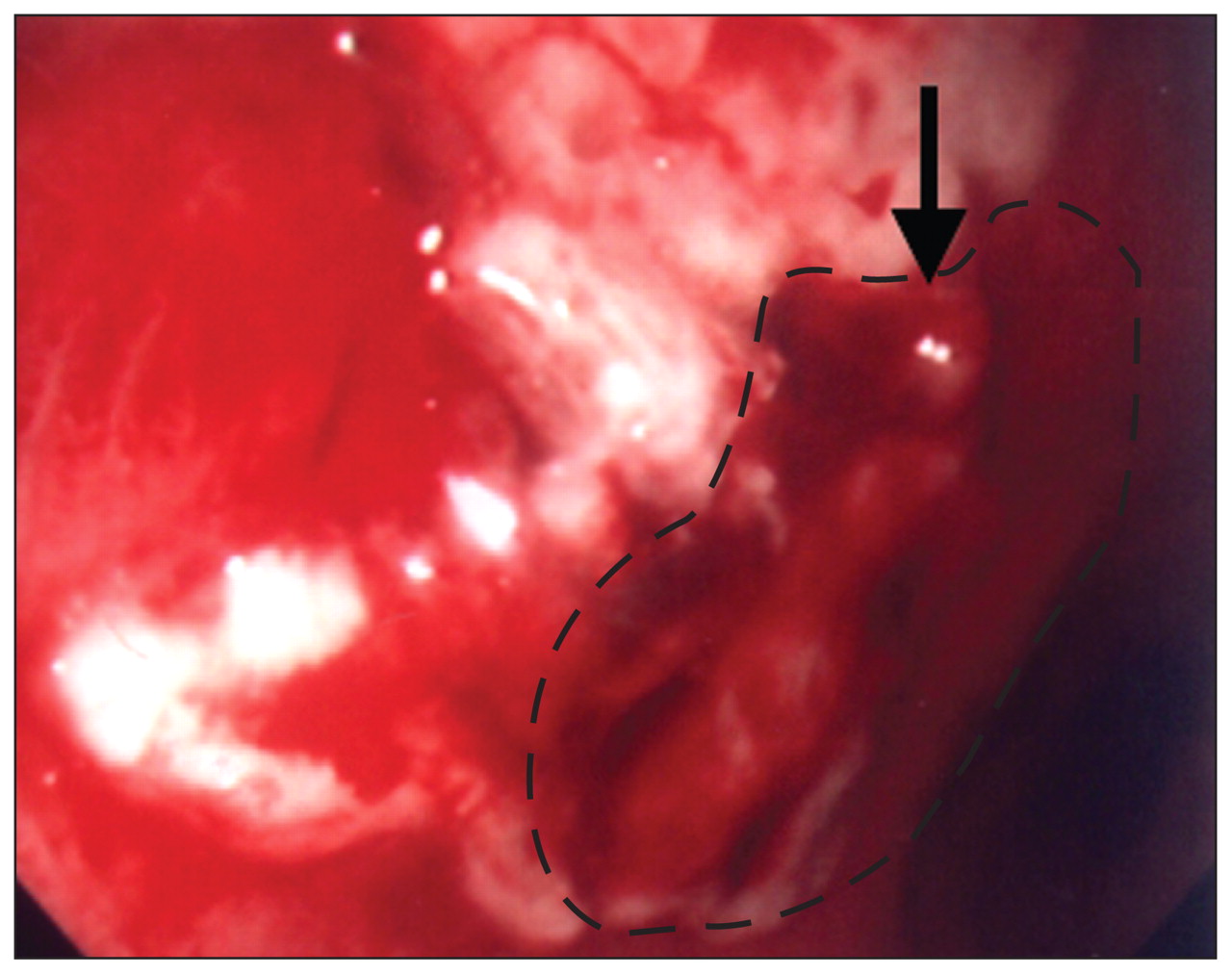
A colonoscopy following gentle rectal irrigation showed several hard fecalomas inside the ascending colon and transverse colon, and a large, irregular ulcer with active bleeding from a visible vessel within the ulcer base in the rectum (Figure 2). Endoscopic hemostasis with epinephrine injection was successfully performed. Biopsy specimens taken from the ulcer showed chronic and acute inflammation. The patient was discharged on the twelfth day after admission. One month later, a follow-up sigmoidoscopy demonstrated a normal rectum without recurrent bleeding.

{kind=link}
{kind=link}
Endoscopic image showing a large, irregular ulcer (outlined) with a bleeding visible vessel (arrow) in the rectum.
Stercoral ulceration, first described in 1894,1 is thought to be secondary to inspissated or impacted feces causing pressure necrosis of the bowel wall. It usually occurs in elderly patients with a history of chronic constipation. The prevalence of stercoral ulceration is unknown. In autopsy studies, stercoral ulceration has been found in 1.3%–5.7% of elderly patients in long-term care facilities.2 The lesions commonly occur in the rectum and sigmoid colon along the antimesenteric margin. This pattern is thought to be caused by harder consistency of the stool, relatively poor blood supply, a narrow diameter and high intraluminal pressure in this location. Complications of stercoral ulceration include bleeding and perforation. The diagnosis of nonperforating stercoral ulceration is usually based on the endoscopic finding of an irregular, geographically outlined ulcer that conforms to the contour of the impacted feces. Bleeding from stercoral ulcers has been successfully treated with endoscopic hemostasis, including endoscopic multipolar electrocoagulation and injection therapy.3,4 Surgical intervention is indicated if stercoral perforation or failure to control bleeding is encountered.
Footnotes
-
Competing interests: None declared.
-
This article has been peer reviewed.