


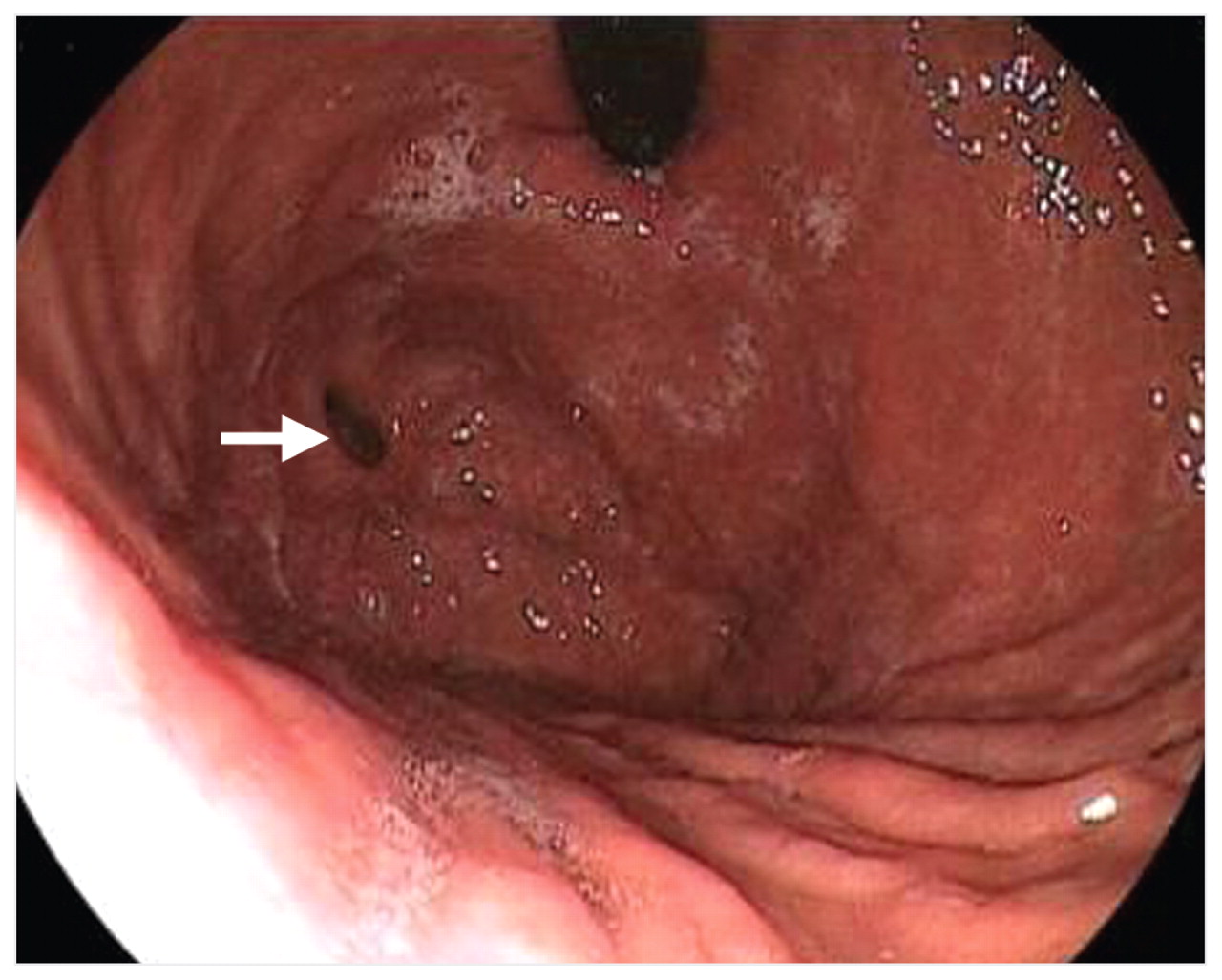
A 58-year-old man presented with a one-month history of upper abdominal pain and anorexia. There was no history of dysphagia, vomiting, hematemesis, melena, tiredness or jaundice. His complete blood count, renal function and liver enzyme levels were normal, as were the results of ultrasonography of the abdomen. An upper gastrointestinal endoscopic scan showed a diverticulum in the fundus of the stomach (Figure 1). The pain was reproduced by probing the diverticulum with biopsy forceps as well as by insufflating it with air. The patient’s symptoms improved after four weeks’ therapy with proton pump inhibitors.

Figure 1: Upper gastrointestinal endoscopic scan showing a diverticulum (arrow) in the fundus of the stomach.
Discussion
Gastric diverticula are uncommon, the rates of detection by endoscopy ranging from 0.01%–0.11%. 1 They usually occur in middle-aged people, with equal distribution among men and women, and can be congenital or acquired. 1,2 Areas of weakness caused by splitting of the longitudinal muscle fibres, an absence of peritoneal membrane and perforating arterioles may predispose to the formation of a diverticulum.
Gastric diverticula are often single, varying in size from 1 to 3 cm. However, multiple and larger diverticula have also been noted, usually adjacent to the gastroesophageal junction and along the lesser curvature or posterior gastric wall. 2 Gastric cardia diverticula may simulate a left adrenal mass; those on the posterior wall could herniate through the dorsal mesentery and fuse with the left posterior body wall. 3
Patients with gastric diverticula are often asymptomatic, although they may present with dyspepsia, vomiting and abdominal pain. Complications such as ulceration, perforation, hemorrhage, torsion and malignancy are uncommon. 2,4 The condition is diagnosed incidentally by radiologic or endoscopic examination. There is no specific treatment required for an asymptomatic diverticulum. 2
Surgical resection is recommended when the diverticulum is large, symptomatic or complicated by bleeding, perforation or malignancy. Both open and laparoscopic resection yield good results. Perioperative gastroscopy can help locate the diverticulum in difficult situations. Laparoscopic access to the posterior aspect of the gastric fundus is possible after the gastrocolic ligament has been divided. 1
Footnotes
-
Previously published at www.cmaj.ca
Competing interests: None declared.
In this issue

{kind=link}
Article tools






Related Articles
Cited By...
- No citing articles found.
More in this TOC Section
Similar Articles
Collections

