


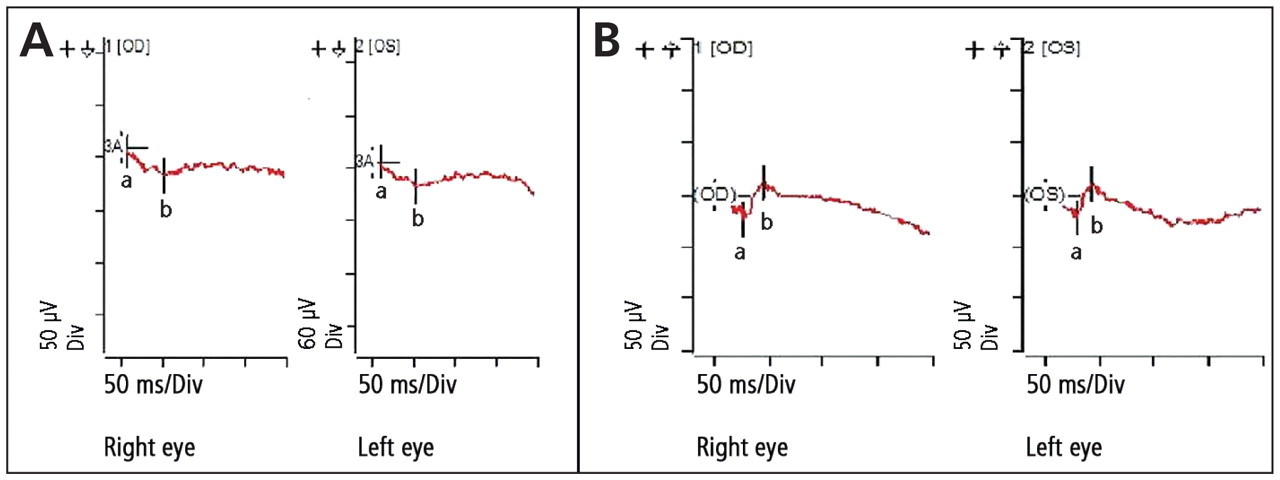
A 58-year-old woman was referred by her optician because of decreased clarity of vision in both eyes with poor night vision. Her medical history included late-stage primary biliary cirrhosis. Her visual acuity was 6/6 in both eyes and ocular examination was unremarkable. An electroretinogram showed a reduced amplitude scotopic (dark-adapted) response (Figure 1A) with a normal photopic (light-adapted) response. This finding suggested a vitamin A deficiency, and subsequent testing showed serum vitamin A levels were low at 0.3 (normal 0.7–1.7) μmol/L. She was given high-dose vitamin A supplementation orally with improvement in her symptoms and electroretinogram trace (Figure 1B).

Figure 1: (A) Dark-adapted electroretinogram showing flattened a and b waves in a 58-year-old woman with decreased clarity of vision and poor night vision. (B) Electroretinogram showing improvement in a- and b-wave amplitude after treatment with vitamin A supplementation.
Because of malabsorption of fat-soluble vitamins, vitamin A deficiency occurs in 33% of patients with primary biliary cirrhosis. 1 Retinol is the most active form of vitamin A in the body. In the rod cells of the retina, all-trans retinol is converted into 11-cis retinol, which then combines with a membrane-bound protein called opsin to yield rhodopsin. Rhodopsin is essential for phototransduction, especially in low-light conditions. 2 Thus patients with vitamin A deficiency (e.g., from malabsorption in primary biliary cirrhosis or extensive small bowel resection) may present with night blindness.
Electroretinography is primarily used in diagnosing retinal dystrophies and degeneration, evaluating chronic ischemic damage from vascular disease and monitoring drug toxicity (e.g., chloroquine, thioridazine). It is available in most ophthalmology departments. A corneal contact lens electrode is placed on the eye, which is well tolerated by most patients. The presence of cataracts does not appreciably affect testing.
The electroretinogram waveform represents a mass electrical response generated by the entire retina following a brief flash of light. In general, the electroretinogram is characterized by a negative waveform (a wave) representing photoreceptor (rod and cone) response followed by a positive wave-form (b wave) generated by the Müller cells and bipolar cell layer.
In photopic electroretinography, the patient stays in a light-adapted state and the retina is stimulated with a bright flash of light. The rods are thus suppressed by light adaptation and do not contribute to the waveform. The result is primarily a cone response with prominent a and b waves, and the results of this test were normal in our patient.
Because rods are 1000 times more sensitive to light than cones, dark-adapted testing or scotopic electroretinography is done by dark-adapting the patient’s eyes for 20 minutes and then stimulating the retina with a dim light below the cone threshold. 3 The resulting waveform normally has a prominent b wave and a minimal a wave. Because of rod dysfunction, vitamin A deficiency shows a flat scotopic electroretinogram, as was evident in our patient.
Footnotes
-
Previously published at www.cmaj.ca
This article has been peer reviewed.
Competing interests: None declared.
Acknowledgement: The authors thank Mr. Paul Gerry for his help in obtaining electroretinograms.
In this issue
{kind=link}
Article tools






Jump to section
Related Articles
Cited By...
- No citing articles found.
More in this TOC Section
Similar Articles
Collections

