


- © 2008 Canadian Medical Association
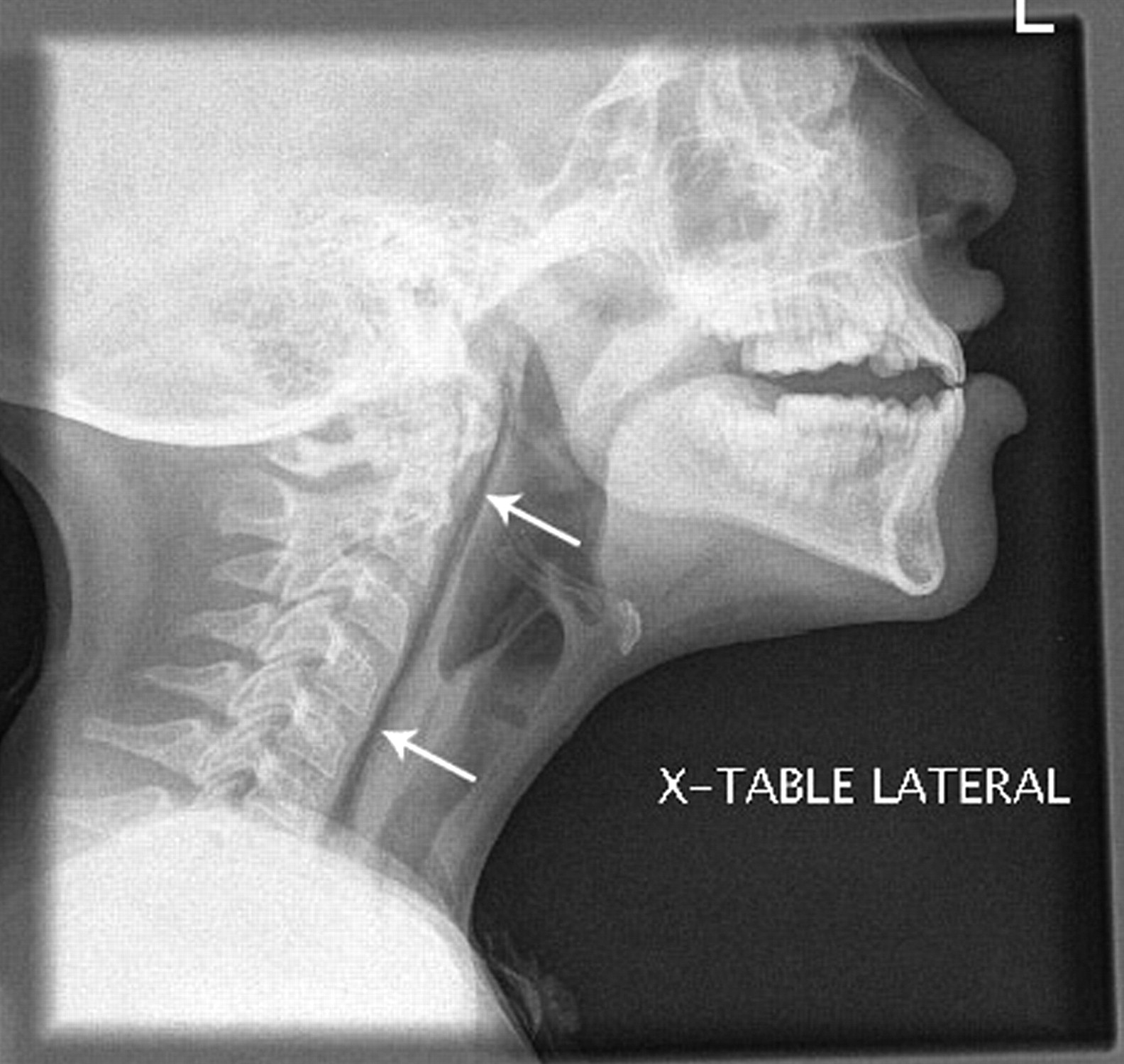
A 10-year-old girl presented with a 3-day history of vomiting, diarrhea and sore throat. She had no history of fever, chest pain, respiratory distress, weight loss or travel. On examination, she was mildly tachycardic with normal blood pressure, temperature, respiratory rate and oxygen saturation in room air. She was drooling and had limited range of motion in her neck. Bloodwork was consistent with dehydration and showed elevated levels of sodium, urea, creatinine and hemoglobin, and an elevated hematocrit. A lateral radiograph of her neck showed air in the retropharyngeal space with no evidence of soft-tissue swelling (Figure 1). A radiograph of her chest revealed small bilateral pneumothoraces and pneumomediastinum tracking into her neck and right shoulder (Figure 2). Results of contrast studies were normal.

Figure 1: Radiograph of the neck of a 10-year-old girl showing air in the retropharyngeal space (arrows) with no evidence of soft-tissue swelling.

Figure 2: Radiograph of patient's chest showing small bilateral pneumothoraces and pneumomediastinum (arrows) tracking into her neck and right shoulder.
What is your diagnosis?
a. Rupture of the esophagus (Boerhaave syndrome)
b. Spontaneous retropharyngeal emphysema
c. Retropharyngeal abscess
d. Traumatic penetrating injury
Discussion
The answer is (b) spontaneous retropharyngeal emphysema, a diagnosis of exclusion that is most often associated with a pneumomediastinum. Air dissects through tissue planes from the mediastinum into the neck.1 Causes of the condition include explosive coughing, singing, weight lifting, labour and vomiting, all of which increase intrathoracic pressure.2 Patients usually present with dysphagia, sore throat and neck pain. Physical examination may reveal subcutaneous emphysema in the neck and chest. If there is also pneumomediastinum, the patient may have dysphonia and retrosternal pain on examination, and Hamman sign (a crunching sound heard over the chest in cases of mediastinal emphysema). Hamman sign is classically described during systole and is often transient.3
Conservative treatment, including bed rest, observation, analgesia and therapy with 100% oxygen to increase the resorption gradient for nitrogen, is often sufficient.4 With this treatment, most cases resolve within 5 to 7 days depending on the severity of injury. Therapy with 100% oxygen is most useful when patients have respiratory distress or discomfort. Antibiotics are not needed unless there are signs of infection.
Differential diagnosis: Although spontaneous retropharyngeal emphysema is usually a benign process with a good prognosis, other causes of retropharyngeal emphysema should be ruled out (Table 1). These causes, including infection, trauma caused by intubation or foreign-body ingestion and esophageal perforation (Boerhaave syndrome), require further investigation with contrast studies, endoscopy, or urgent surgical consultation and intervention.
Table 1.
Boerhaave syndrome, a spontaneous perforation of the esophagus, was first described in 1724.5 This syndrome must be ruled out before a diagnosis of spontaneous retropharyngeal emphysema can be made. In our patient's case, we performed contrast studies that showed no esophageal perforations.
Retropharyngeal emphysema can result from an infectious process in the retropharyngeal area, such as retropharyngeal abcess.6 Clinical signs, such as fever or leukocytosis, can be helpful in making this diagnosis. Also, neck imaging may reveal a thickened retropharyngeal space.
A history of traumatic penetrating injury from such causes as foreign-body impaction, intubation or esophageal instrumentation helps to guide further investigations, including contrast studies.6
Footnotes
-
CMAJ invites contributions to the Clinical Quiz column, which uses multiple-choice questions to guide a focused image-based discussion of the diagnosis or management of clinical cases. Submit manuscripts online at http://mc.manuscriptcentral.com/cmaj.
Competing interests: None declared.
In this issue

{kind=link}
{kind=link}
Article tools






Related Articles
Cited By...
- No citing articles found.
More in this TOC Section
Similar Articles
Collections

