


- © 2008 Canadian Medical Association
A 53-year-old man from Texas presented with a 2-month history of malaise, anorexia and 14-kg weight loss, and a 2-week history of chest pain and a productive cough of yellow–brown sputum. He was a smoker (40 pack-year), and he had hypertension, hepatitis C and a long history of alcohol abuse (4–6 beers per day for > 25 years). He denied having fever, chills, night sweats, dyspnea or hemoptysis. His vital signs were normal, and physical examination revealed temporal wasting, pallor, poor oral hygiene with multiple cavities, wheezing and decreased breath sounds in the right lung, and clubbing of his fingers and toes. He had mild normocytic anemia and hypoalbuminemia. He was HIV negative. A chest radiograph showed a mass in the lower lobe of his right lung and a loculated effusion in the right pleura (Figure 1). A computed tomography scan of his chest revealed a 2.5 × 2.9-cm spiculated mass, pleural effusion on the right side, mediastinal lymphadenopathy and postobstructive pneumonia (Figure 1). The results of extensive imaging tests for metastatic disease, including computed tomography scans of his head, abdomen and pelvis and a bone scan, were negative.
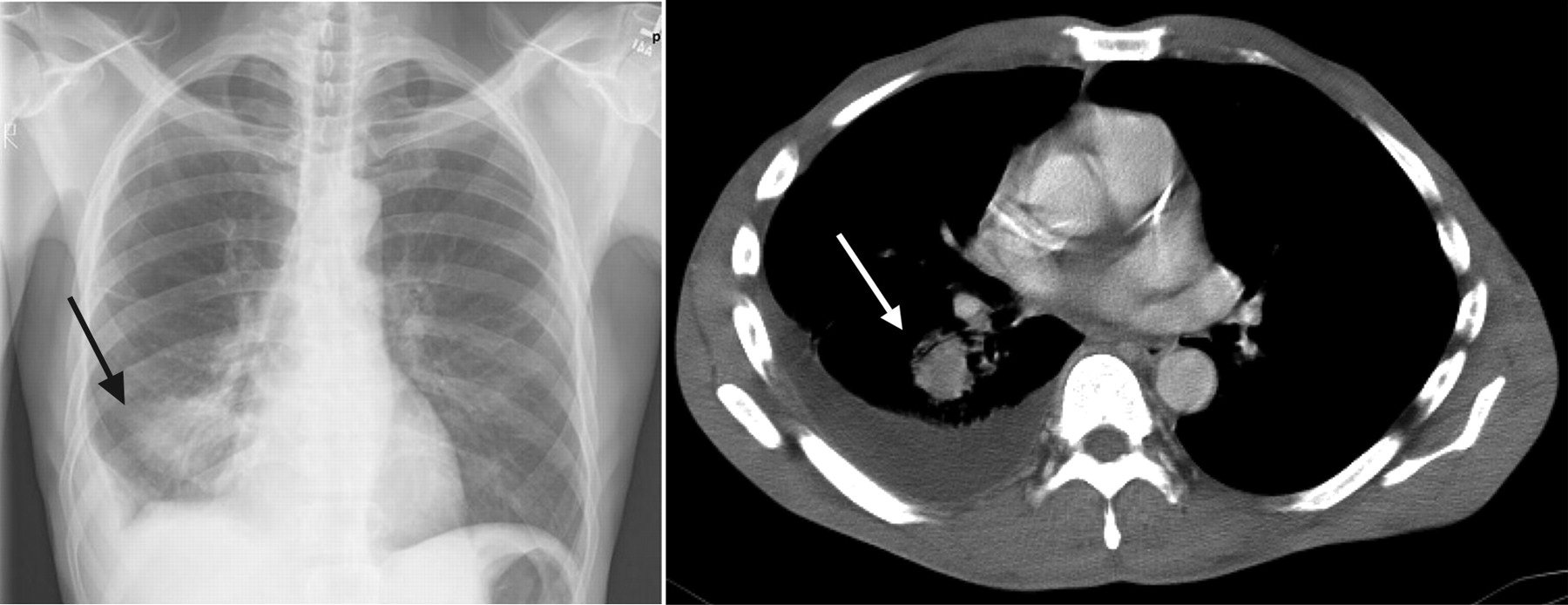
Figure 1: A chest radiograph (left) of a 53-year-old man showing a mass (arrow) in the lower lobe of his right lung, and a computed tomography scan of his chest (right) revealing a 2.5 × 2.9-cm spiculated mass (arrow), pleural effusion on the right side, mediastinal lymphadenopathy and postobstructive pneumonia.
What is the diagnosis?
a. Pulmonary tuberculosis
b. Lung cancer
c. Pulmonary actinomycosis
d. Pulmonary nocardiosis
e. Pulmonary blastomycosis
Discussion
Although the most likely diagnosis in a smoker who presents with the clinical and radiographic manifestations we described would be lung cancer, in our patient the answer is (c) pulmonary actinomycosis. We performed a bronchoscopy and an endoscopic ultrasound biopsy of paratracheal lymph nodes, but the results did not reveal the diagnosis. We also performed mediastinoscopy, video-assisted thoracoscopic surgery and decortication of the right pleura. The results of all biopsies were negative for malignant disease. The results of routine, fungal and acid-fast bacilli cultures were also negative. The pathological specimen from the pleura showed extensive neutrophilic infiltration and sulfur granules (Figure 2) as well as branching micro-organisms consistent with Actinomyces (Figure 3). The patient's symptoms resolved after a 6-month course of amoxicillin. A subsequent radiograph of his chest showed improvement (Figure 4). The patient remained asymptomatic 2 years after the completion of treatment and showed no evidence of relapse.

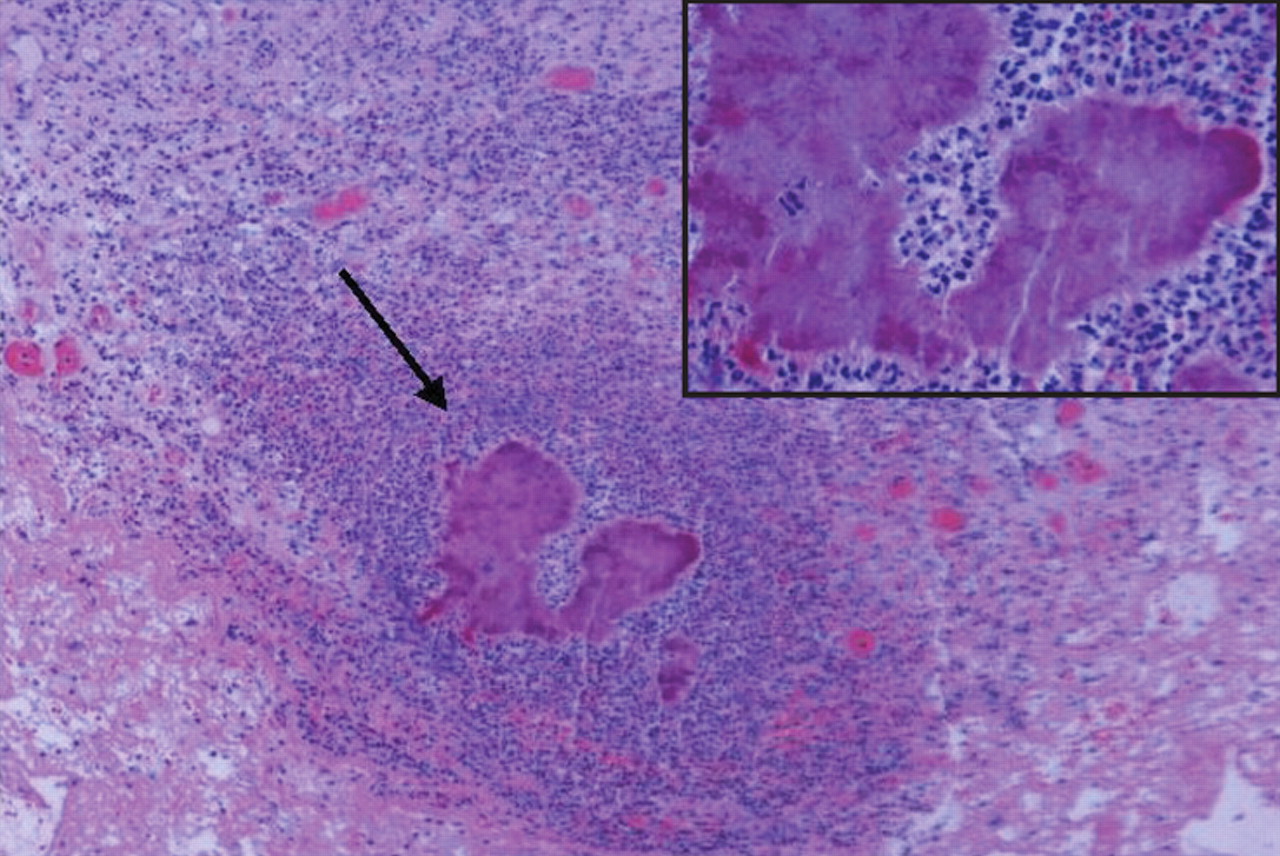
Figure 2: Histological section of the specimen from the right pleura showing extensive neutrophilic infiltration and sulfur granules (arrow and inset). Hematoxylin and eosin stain, original magnification × 100.
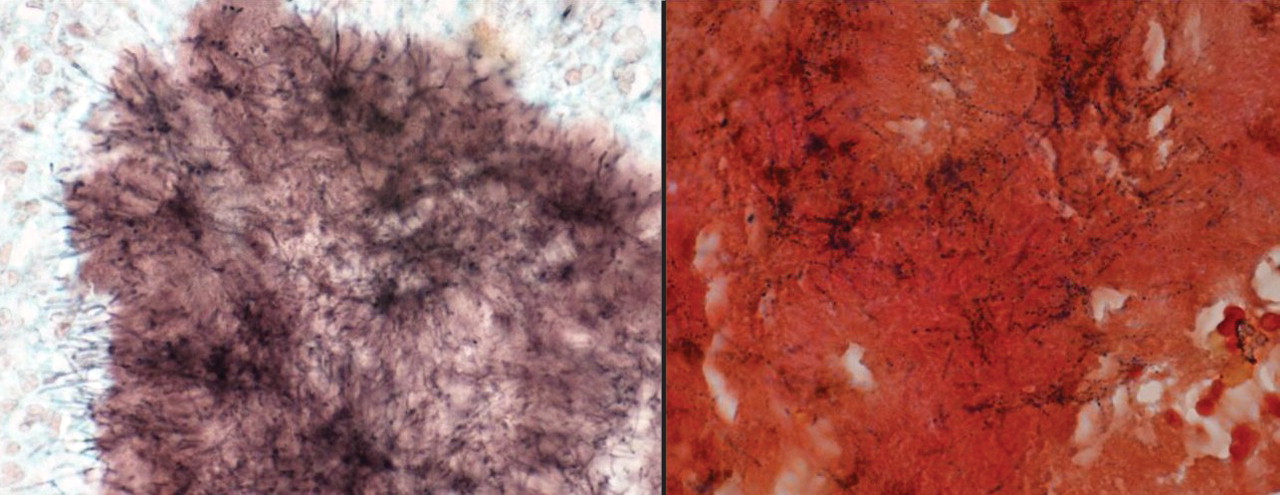
Figure 3: Histological sections of pleural specimen showing branching micro-organisms consistent with Actinomyces. Left: Gomori methenamine silver stain, original magnification × 400. Right: Gram stain, original magnification × 1000.

Figure 4: Radiograph of the patient's chest showing improvement after a 6-month course of amoxicillin.
Pulmonary actinomycosis: Pulmonary actinomycosis is rare.1 It accounts for 10%–15% of reported cases of actinomycosis and occurs less frequently than the cervicofacial and abdominopelvic forms of the disease.1,2 It is caused by Actinomyces, a genus of gram-positive anaerobic micro-organisms that are susceptible to several classes of antibiotics, including penicillin G (the antibiotic of choice) and other β-lactams, clindamycin, tetracycline and macrolides.1,2 Although Actinomyces israelii is by far the most common species found in humans, Actinomyces meyeri is more frequently seen in cases of pulmonary actinomycosis.1,2 Important risk factors for pulmonary actinomycosis include poor dental hygiene and alcohol abuse, both of which were present in our patient. These risk factors predispose patients to aspirate oral secretions containing Actinomyces bacteria into the lower respiratory tract.1,2
The clinical presentation and radiographic features of pulmonary actinomycosis closely resemble those of lung cancer and chronic suppurative pulmonary infections such as tuberculosis and fungal infections.2 Therefore, the diagnosis of pulmonary actinomycosis is challenging and often delayed. Weese and Smith reported that the average time from symptom onset to diagnosis was 6 months, and the infection was suspected at the time of admission in less than 10% of cases that were later diagnosed as pulmonary actinomycosis.3 Pulmonary actinomycosis should be suspected in patients with known risk factors (e.g., alcohol abuse, poor dental hygiene) who present with nonspecific, subacute, or chronic constitutional and respiratory symptoms. Clinical features that can point to a diagnosis of pulmonary actinomycosis in such patients include the development of draining sinus tracts, and radiographic features include the presence of pulmonary abnormalities that progress across different anatomic planes.
For a definitive diagnosis of actinomycosis, the presence of sulfur granules in cultures or biopsy material is required. In tissues, Actinomyces species grow in filamentous clusters surrounded by polymorphonuclear neutrophils, as shown in Figure 2 and Figure 3. When these clusters exude from soft tissues through sinus tracts, they are macroscopically yellow, and are called sulfur granules. In rare cases, Actinomyces species can be identified in blood cultures.1 A prolonged course (6–12 months) of antibiotics is necessary to treat pulmonary actinomycosis and is usually successful if started early.2 Thus, pulmonary actinomycosis should be suspected in patients who initially receive a diagnosis of community-acquired pneumonia and respond to antimicrobial therapy but who promptly relapse after completion of a short course of antibiotics.
Differential diagnosis: As mentioned previously, the clinical and radiographic presentation of chronic lung infections and lung cancer may be similar to that of pulmonary actinomycosis (Table 1).1,2 We ruled out lung cancer in our patient because the results of multiple tissue biopsies obtained during bronchoscopy and decortication of the pleura were negative.
Table 1.
Reactivation of pulmonary tuberculosis typically affects the upper lobes of the lungs. This was not the case in the radiographs of our patient, whose acid-fast bacilli cultures were also negative.
Pulmonary nocardiosis usually affects immunocompromised patients. It is caused by Nocardia species — gram-positive branching filamentous rods that resemble Actinomyces species. Unlike Actinomyces species, the presence of Nocardia species is detected with the modified acid-fast Kinyoun stain.4
Finally, pulmonary blastomycosis is an endemic mycosis that can also masquerade as lung cancer.5 However, the absence of a relevant travel history, the absence of blastomycosis in Texas and the negative fungal cultures in our patient made this diagnosis unlikely.
Footnotes
-
CMAJ invites contributions to the Clinical Quiz, which uses multiple-choice questions to guide a focused image-based discussion of the diagnosis or management of clinical cases. Submit manuscripts online at http://mc.manuscriptcentral.com/cmaj.
This article has been peer reviewed.
Competing interests: None declared.
In this issue

{kind=link}
{kind=link}
{kind=link}
{kind=link}
Article tools






Jump to section
Related Articles
Cited By...
- No citing articles found.
More in this TOC Section
Similar Articles
Collections

