


- © 2007 Canadian Medical Association
What's your call?

CT scan of the lumbar spine of a 26-year-old man from India who presented with low back pain, fever and weight loss of 3 weeks' duration.
A 26-year-old man from India who had lived in France for 1 year experienced low back pain, fever and weight loss. After 3 weeks of it, he came to hospital. His medical history included kidney stones and alcohol abuse, but was negative for tuberculosis. He denied having any weakness or numbness of the lower limbs, and the results of a neurologic examination were normal. HIV test results were negative. Plain radiographs appeared normal. However, a CT scan of the spine revealed multiple lytic, well-defined osseous lesions, with surrounding sclerosis and central opacity disseminated in his lumbar vertebrae and sacrum (Figure 1; additional images available online at www.cmaj.ca/cgi/content/full/177/2/148-a/DC1). We observed no disc extensions or soft-tissue abscesses. A technetium-99 bone scan showed no hyperfixation of the lesions, although some found on the sacrum and right ilium via CT showed hyperfixation with positron emission tomography.
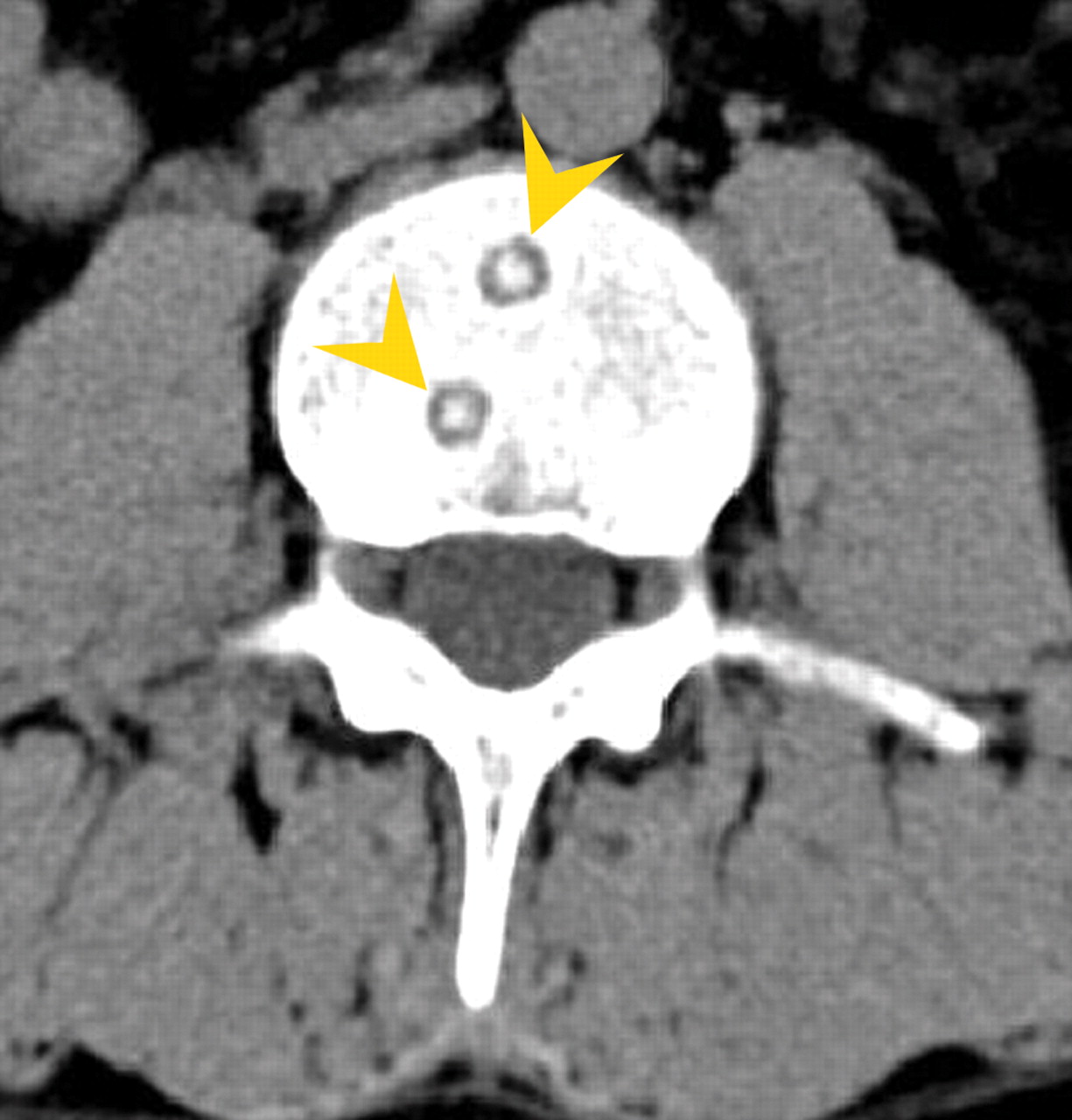
Figure 1: An axial reconstruction of a CT scan of the lumbar spine (the L3 vertebra, in this image), with use of a soft-tissue filter. Small, round, lytic bone lesions were found with well-defined margins, surrounding sclerosis and central opacity (arrowheads). This central opacity is called a button sequestrum sign.
Specimens of the L5 vertebral body obtained via percutaneous biopsy showed several tuberculous granulomas with a central mass of epithelioid cells, some giant cells and surrounding lymphocytes with no caseous focus. No acid-fast bacilli were found in the specimen, and cultures remained negative. Nevertheless, a specimen biopsied from an enlarged cervical lymph node yielded acid-fast bacilli later identified as Mycobacterium tuberculosis. A diagnosis of disseminated tubercular oste-itis (cystic tuberculosis) with sequestra was made.
The patient underwent 2 months of daily chemotherapy with isoniazid (300 mg), pyrazinamide (15– 30 mg/kg), rifampin (600 mg) and ethambutol (15 mg/kg), followed by 22 months of daily isoniazid (300 mg) plus rifampin (600 mg). He also wore external bracing for the first 8 months of his treatment. His clinical course was favourable, and his back pain completely resolved within 5 weeks. Although a CT scan 6 months after the biopsies showed the same bone lesions at the same size, their sclerotic margins were thicker, a possible sign of cicatrization. At that time, there had been no sign of recurrence.
Osteoarticular tuberculosis occurs in 2.5%– 5% of tuberacular infections; of these, 50%–60% are vertebral, most frequently in lower thoracic and lumbar regions. They result from an arterial hematogenous seeding.
An opaque, radiodense centre in a lytic lesion is called a button sequestrum sign. Originally described as a manifestation of eosinophilic granuloma,1 the sign may also be seen in cases of osteomyelitis, fibrosarcoma or lymphoma.2 The pathophysiology of tuberculous osteomyelitis is believed to involve granulation tissue initially formed in the marrow, with secondary resorbtion of trabeculae. Caseous necrosis creates an abscess cavity that contains pus and small granules of bone. The abscess is surrounded by granulation tissue, connective tissue with cellular elements and sclerotic trabeculae.2,3 Radiographs show foci of oste-olysis, with condensation and periostitis. Sequestrum formation may manifest as a central increase in radiodensity within the lytic area, producing the button sequestrum sign.
Footnotes
-
This article has been peer reviewed.
Acknowledgements: We thank Drs. Myriam Diemer, Karine Champion and Valerie Bousson for their help in the preparation of this manuscript.
Competing interests: None declared.
In this issue

{kind=link}
Article tools






Related Articles
Cited By...
- No citing articles found.
More in this TOC Section
Similar Articles

