


The Case: A 70-year-old man came to the emergency department with a complaint of dysphagia of acute onset. He reported a similar episode a week earlier that had resolved without treatment.
His history included mild cognitive impairment, a remote-left-hip arthroplasty, hip and knee osteoarthritis, and a recent hospital admission for a pelvic fracture that had not required surgical correction. His only medication was acetaminophen. There was no family history of neurologic or autoimmune disorders. The patient denied any diplopia or focal weakness.
Physical examination revealed a healthy-seeming man with a normal heart rate and blood pressure. Cranial nerve examination failed to disclose fatigable diplopia or ptosis. His muscle strength and bulk were normal in both upper and lower extremities. His reflexes were symmetric; plantar response was downgoing. Sensory modalities were intact.
Clinical swallowing trials showed signs consistent with a pharyngeal dysphagia, including multiple secondary swallowing efforts, nasal regurgitation, an occasional gurgling voice after swallowing, and frequent throat clearing and coughing during and after swallow trials. Abnormal oral motor findings included fluctuating hypernasality and occasional blocking dysfluencies — sharp interruptions of airflow or phonation that impaired speech. MRIs of the brain and brainstem appeared normal.
The patient underwent videofluorography before and after receiving edrophonium (Tensilon) intravenously. Edrophonium is a short-acting anticholinesterase that prolongs the presence of the neurotransmitter acetylcholine at the neuromuscular junction. Videofluoroscopic assessment after its administration revealed a dramatic improvement in swallow function (Fig. 1; a video is available at www.cmaj.ca/cgi/content/full/175/10/1203/DC1). Striking improvements were noted in all parameters, including velopharyngeal closure, base-of-tongue retraction, epiglottic deflection and pharyngeal propulsion. No laryngeal penetration was seen.
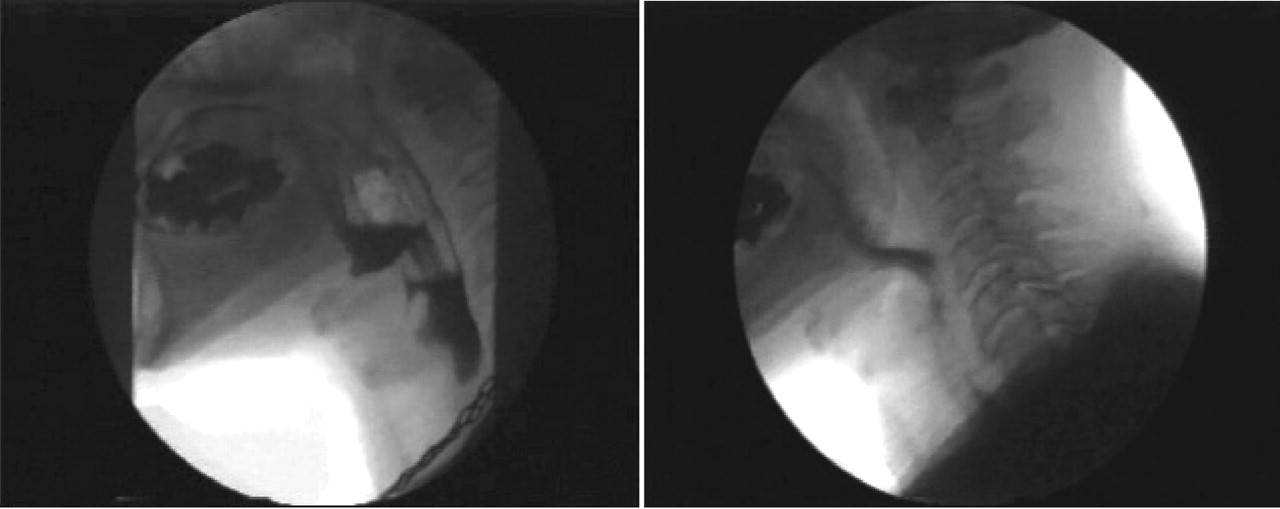
Fig. 1: Imaging results during the Tensilon test. Videofluorographs before (left) and immediately after an intravenous administration of 10 mg of edrophonium. The patient's swallowing mechanism showed a rapid and complete recovery in all aspects (right) after receiving the acetylcholinesterase inhibitor. Because edrophonium is a short-acting, the response is transient and useful only as a test.
These dramatic improvements subsided quickly: swallow trials repeated 4– 5 minutes after the edrophonium administration revealed a rapid re-emergence of severe pharyngeal dysphagia. Single-fibre electromyography (SFEMG) confirmed the presence of a neurotransmission dysfunction consistent with myasthenia gravis (Fig. 2). CT scans of the patient's chest and mediastinum revealed no abnormalities.

Fig. 2: SFEMG (single-fibre electromyography) of a normal control (left) and our patient with myasthenia gravis. Increased variability (known as “jitter”) in our patient (right) was consistent with a neurotransmission abnormality.
The patient was given a course of oral pyridostigmine, to which he had a partial response. Prednisone was added to the regimen, after which his swallowing returned to normal. Six months after the initial diagnosis, the patient is symptom-free; an attempt to taper the steroid is currently underway.
Myasthenia gravis (MG) is an uncommon autoimmune disease (Box 1) in which IgG antibodies directed against the acetylcholine receptors at the neuromuscular junction prevent normal muscle contraction and lead to muscle weakness. Originally described (or thought to be described) in a patient with dysarthria, MG is now thought of as the classic autoimmune disease.1

The thymus is probably involved in the pathogenesis of MG;1 thymic tumours should therefore be excluded. Between 30% and 60% of patients with epithelial thymic tumours (thymoma) have MG and, in turn, some 10%–15% of people with MG have thymoma. Their relationship has yet to be fully elucidated, although the initial steps in the pathogenesis of MG in most cases take place within abnormal thymic microenvironments, whether inflammatory or neoplastic. In about 90% of patients, no cause can be identified.

The classical presentation includes a myasthenic “snarl” and a voice that sounds nasal because of bulbar and facial muscle weakness (Box 2; Table 1). Dysphagia is the only manifestation of MG that has been well documented:2 about 20% of cases involve the bulbar muscles. MG can be diagnosed by means of serology, nerve conduction studies with SFEMG, or the classic Tensilon test. Since about 85% of patients with generalized disease will have antibodies to the acetylcholine receptor, a positive result is diagnostic for MG; unfortunately, this test is not routinely available.
Table 1.
A long-acting oral anticholinesterase such as pyridostigmine is the first line of treatment. Immunosuppression with prednisone is used when symptom improvement is inadequate; azathioprine or mycophenolate mofetil can also be added. Thymectomy is considered for all patients younger than 55 years who have generalized myasthenia or a resectable thymoma. Plasmapheresis and intravenous immune globulin therapy are reserved for acute exacerbations, when the need is for a rapid benefit.
This case demonstrates the importance of considering neurotransmitter diseases in the approach to new-onset focal weakness that involves the bulbar musculature. MG was diagnosed in our patient, who presented purely with swallowing abnormalities, via videofluorography during a Tensilon test.3 This novel diagnostic approach should be considered for patients with suspected bulbar MG.
Footnotes
-
Acknowledgements: We thank David Chan and Neville Bayer for their feedback on some components of the manuscript.
Competing interests: None declared.
In this issue

{kind=link}
{kind=link}
{kind=link}
{kind=link}
Article tools






Related Articles
Cited By...
More in this TOC Section
Similar Articles

