


Background and epidemiology: At the end of 2002 an estimated 56 000 people in Canada had HIV infection or AIDS.1 Some 2800– 5150 of these people were infected during 2002. The new infections resulted predominantly from men having sex with men (40%), intravenous drug use (34%) and heterosexual encounters (21%). Canadian populations experiencing a growing incidence of HIV infection include women, Aboriginal people and people from countries where HIV is endemic.1 An estimated 17 000 (30%) of the prevalent cases involve people who have not been tested and are unaware of their infection. Screening for HIV infection therefore continues to be a public health priority.1
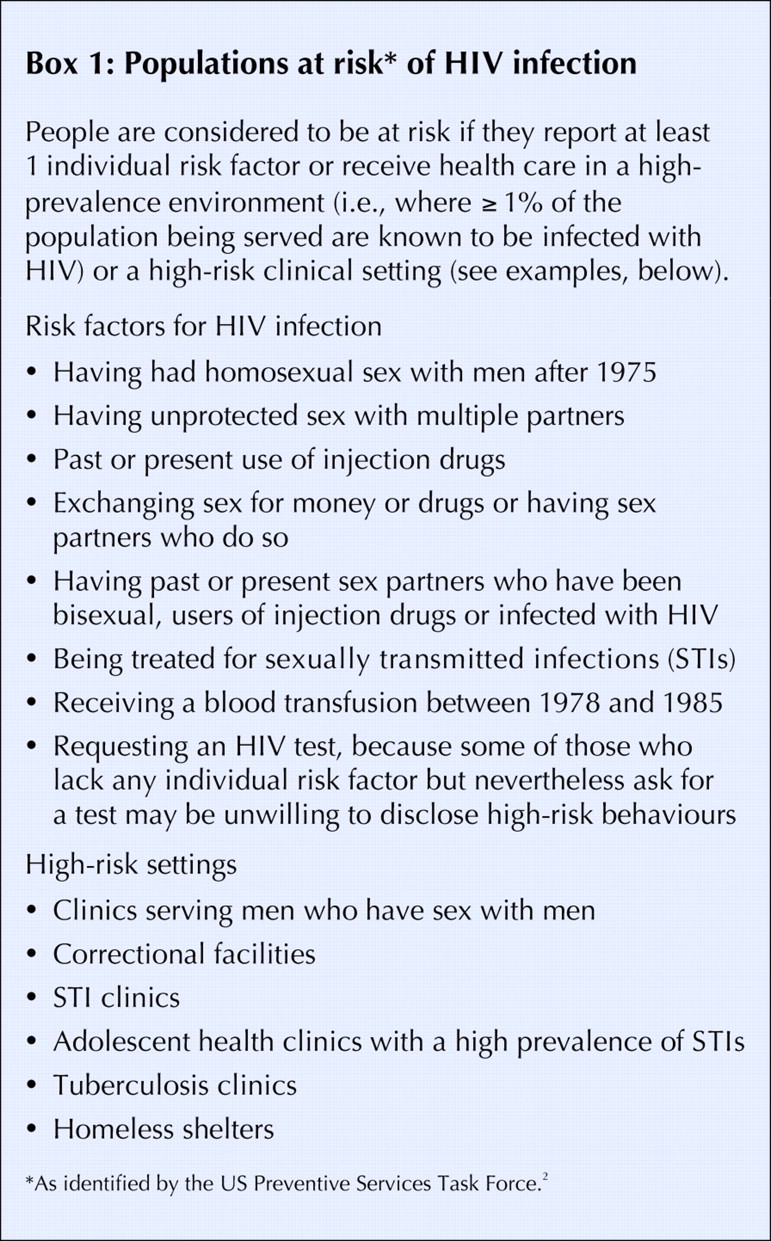
The US Preventive Services Task Force strongly recommends that clinicians screen all at- risk adolescents and adults. The task force recently updated their HIV screening recommendations (Box 1) and supporting scientific evidence.2 The greatest change from the previous set of recommendations is to expand HIV screening to all pregnant women and not just those who are at high risk.

The US task force did not make a recommendation for or against routine HIV screening for adolescents or adults who are not considered to be at risk. Although screening may detect HIV in additional persons who may benefit from treatment, the yield is low and potential harms from screening (e.g., anxiety) are evident.2
The 1998 Canadian STD Guidelines,3 which are currently being updated, include 2 additional risk factors for HIV infection: anal intercourse (receptive contact in particular) and a history of hepatitis B infection. These guidelines suggest that HIV testing should be offered to people with at-risk behaviours, patients with clinical or laboratory clues suggestive of HIV infection, anybody requesting the test and all pregnant women. Children born to mothers who have tested positive for HIV must also be evaluated.3
Clinical management: Whenever HIV screening is conducted, counselling before and after testing should also be provided. All Canadian provinces and territories make non-nominal testing available (i.e., the person ordering the test knows the patient's identity, but uses a code to order it) and nearly all provide nominal or anonymous testing options. The standard test for HIV infection, the repeatedly reactive enzyme immunoassay followed by a confirmatory Western blot or immunofluorescent antibody assay, is very accurate (sensitivity and specificity both ≥ 99%). Rapid HIV testing is also accurate (sensitivity 96%– 100%, specificity > 99.9%),2 but it is not available everywhere in Canada.
Highly active antiretroviral therapy (HAART) with 3 or more antiretroviral agents has been effective in reducing clinical progression and mortality in people with CD4 cell counts lower than 0.200 х 109/L. There is also good support for the use of antibiotics to prevent opportunistic infections.
Prevention: Condom use can prevent sexual transmission of HIV, and needle exchange programs can make intravenous drug use safer. After a suspected unprotected contact (e.g., an occupational exposure or a sexual assault), prompt prophylactic administration of antiretroviral drugs can greatly reduce the risk of HIV transmission.
In seropositive pregnant women, HAART should be started at 14–34 weeks' gestation and continued until delivery by (elective) cesarean section. The therapy regimen should be augmented with 6 weeks of neonatal prophylaxis with zidovudine, and the infant fed formula. In combination, these steps can reduce the risk of vertical transmission from some 14%– 25% to 1%– 2%.2
In this issue
{kind=link}
Article tools






Jump to section
Related Articles
Cited By...
- No citing articles found.
More in this TOC Section
Similar Articles
Collections

