


- © 2005 CMA Media Inc. or its licensors
A previously healthy 89-year-old woman was referred to the plastic surgery service because of a rapidly growing lesion at the base of her right nostril at the nasolabial fold. The patient had had this lesion for several years, and it had begun to enlarge only in the last few months. A previous biopsy had revealed actinic keratosis, and radiography had shown a deviated septum. She had become blind in her right eye in the previous 2 months. She had no history of malignant skin disease, and her only medical history was that of hypothyroidism.

The lesion was draining serosanguinous material, and there was a central area of necrosis surrounded by inflammation. Her blind eye had ptosis and a dilated nonreactive pupil (Fig. 1). A clinical diagnosis of orbital apex syndrome secondary to an invading lesion was made. Punch biopsies showed a squamous cell carcinoma, and a CT scan revealed a large tumour that extended from the orbit into the infratemporal region with destructive changes to the greater sphenoid wing (Fig. 2). Unfortunately, the lesion was not amenable to surgical correction.

Orbital apex syndrome consists of paralysis of the optic, oculomotor, trochlear, abducent and ophthalmic portions of the trigeminal cranial nerve. This leads to the findings of unilateral blindness, fixed dilated pupils, proptosis, ptosis and ophthamalmoplegia. Superior sulcus tumour syndrome is closely related but does not involve the optic nerve. The orbital apex is the most posterior part of the pyramid-shaped orbit (Fig. 3). The superior orbital fissure lies between the greater and lesser sphenoid wings, and it contains several cranial nerves (III, IV, V and VI).1 The optic canal and the cavernous sinus are nearby. The close proximity of these structures means that a small lesion can lead to dramatic clinical findings.
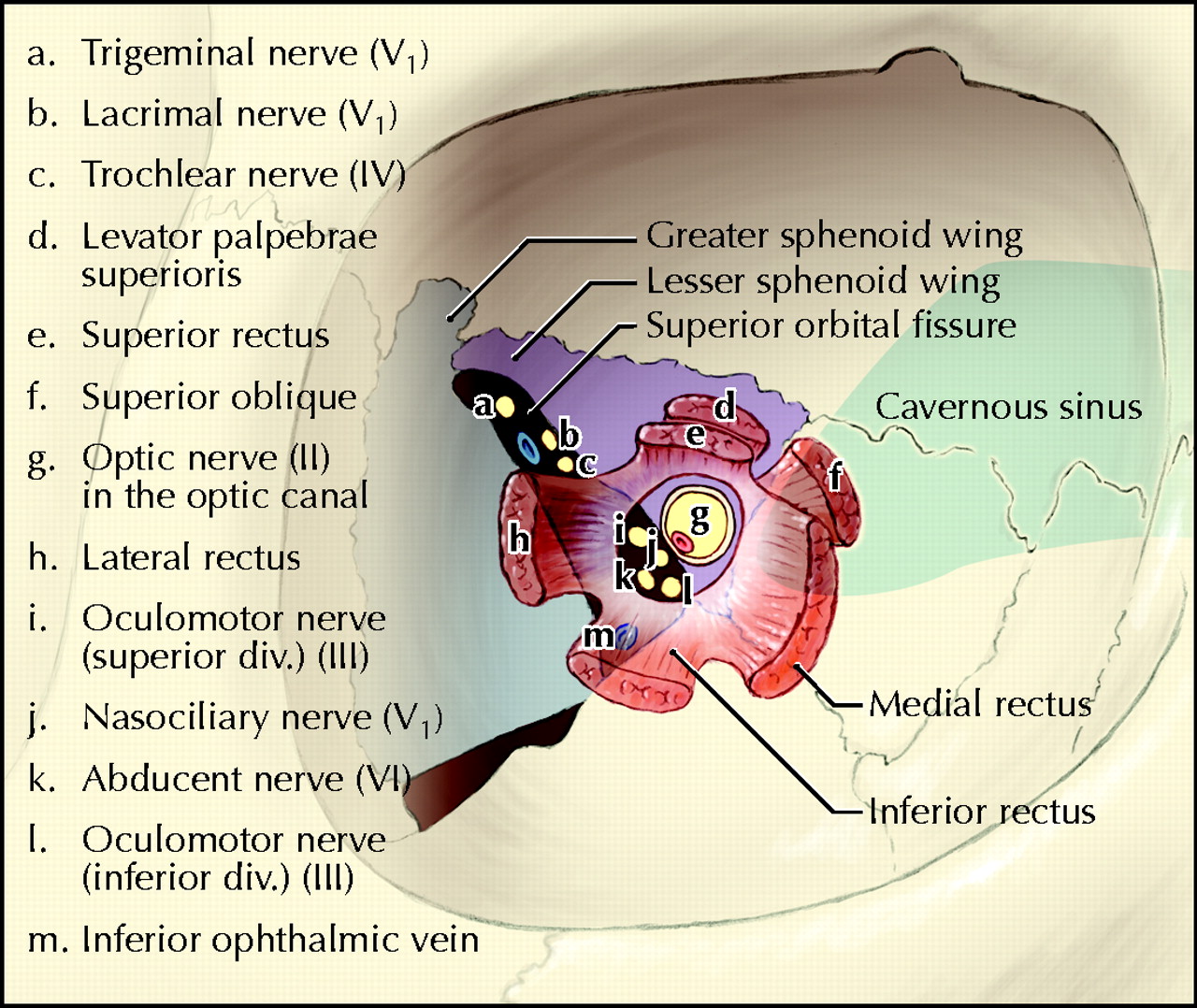
Figure 3. Photo: Lianne Friesen and Nicholas Woolridge
Numerous case reports have been written on orbital apex syndrome. Causes include infection (aspergillosis, tuberculosis, staphylococcus), trauma, sickle cell disease, inflammation, extramedullary hematopoiesis and tumours.2 Primary tumours include optic gliomas, lymphomas and perineural extensions of cutaneous cancers.3 Metastatic disease from the lungs, ovaries and other locations have also been described. Surgery is the primary mode of treatment if the tumour is detected early.
In this issue

{kind=link}
{kind=link}
{kind=link}
Article tools






Jump to section
Related Articles
Cited By...
- No citing articles found.
More in this TOC Section
Similar Articles
Collections

