


- © 2004 Canadian Medical Association or its licensors
A 77-year-old man was taken to his local emergency department with symptoms of ischemic stroke of about 5 hours' duration. He had been speaking and mobilizing normally on waking; however, about 50 minutes later his wife observed that he had returned to bed and was not speaking, but she was unaware that anything was wrong. Two hours later she realized that he was unable to speak and had developed weakness of his right face, arm and leg. At the emergency department, he was alert and could comprehend simple commands but had a severe expressive aphasia. He had normal motor function on the left side but a profound weakness of his right arm (0/5 power) and leg (2/5 power). The plantar reflex was upgoing on the right, and sensation was decreased to all stimuli, but with no signs of visual field neglect. His stroke severity score was 16 out of a possible 42 on the National Institute of Health Stroke Scale (NIHSS). In general, higher scores reflect more severe deficits and a higher probability of death and disability. A baseline head CT scan (not shown) showed early ischemic changes, with loss of grey–white matter differentiation in the left lentiform nucleus.
Because about 5 hours had passed since the patient was last well, he was beyond the normal 3-hour window for the administration of tissue plasminogen activator (tPA). However, after discussing the possible benefits and risks of such therapy in the 3–6-hour window after stroke onset, the family consented to intravenous tPA administration as part of a multicentred research study protocol. MRI scanning of the patient's brain, before and after tPA treatment, was also consented to as part of the study.
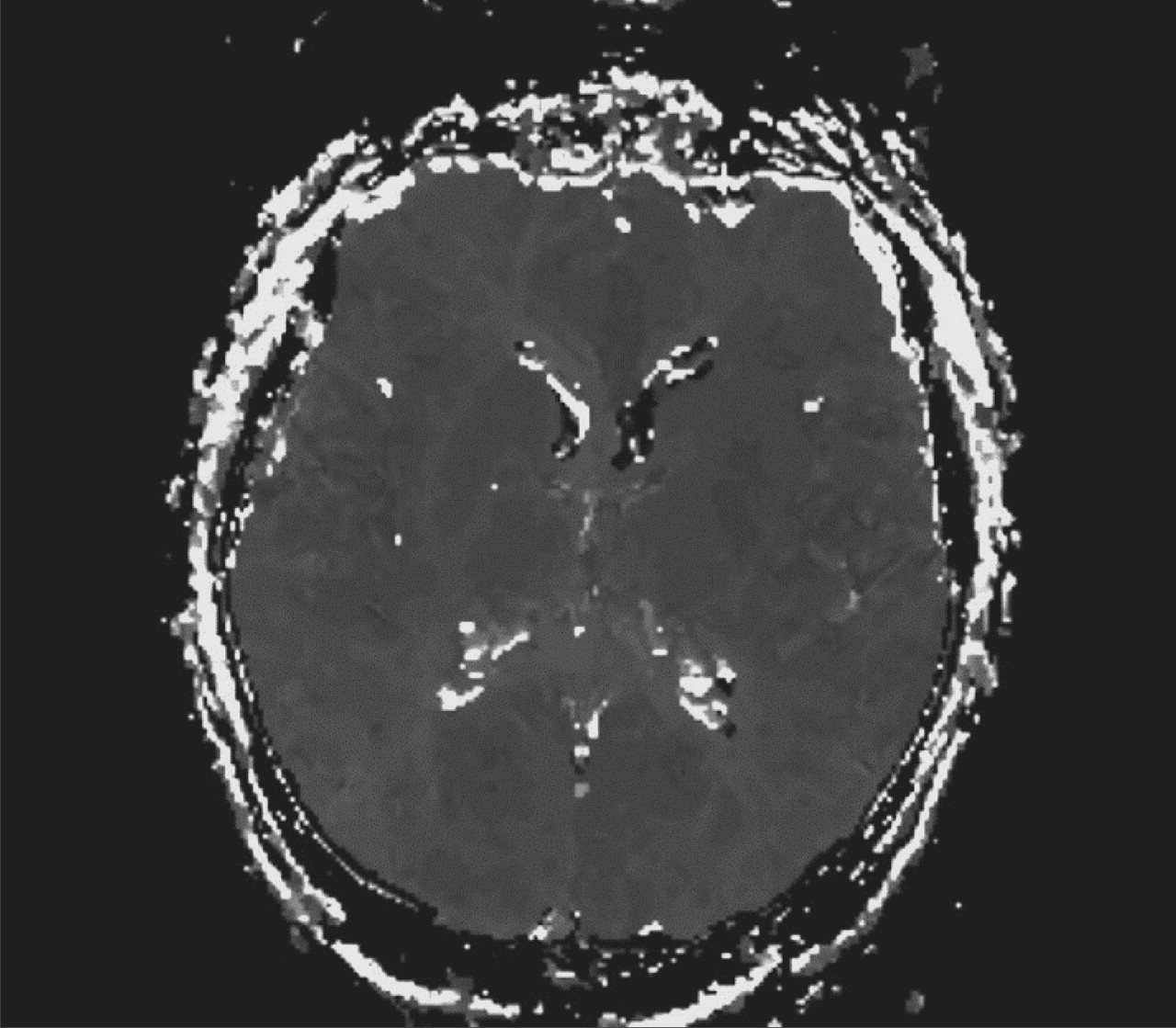
MRI can image both the size of the perfusion defect in the brain (using perfusion-weighted imaging [PWI]) as well as the size of the most severely affected tissue (seen on diffusion-weighted imaging [DWI]). The size of the early PWI defect is a better determinant of clinical outcome and final infarct volume than is the size of the early DWI defect.1 Early ischemic lesions identified on DWI may expand over subsequent hours or days to match the size of the larger PWI defect, with the area of diffusion–perfusion image mismatch representing potentially salvageable tissue. Early resolution of the PWI lesion, which may follow thrombolysis, results in smaller final infarct volumes1 and, as postulated, improved neurological outcomes.
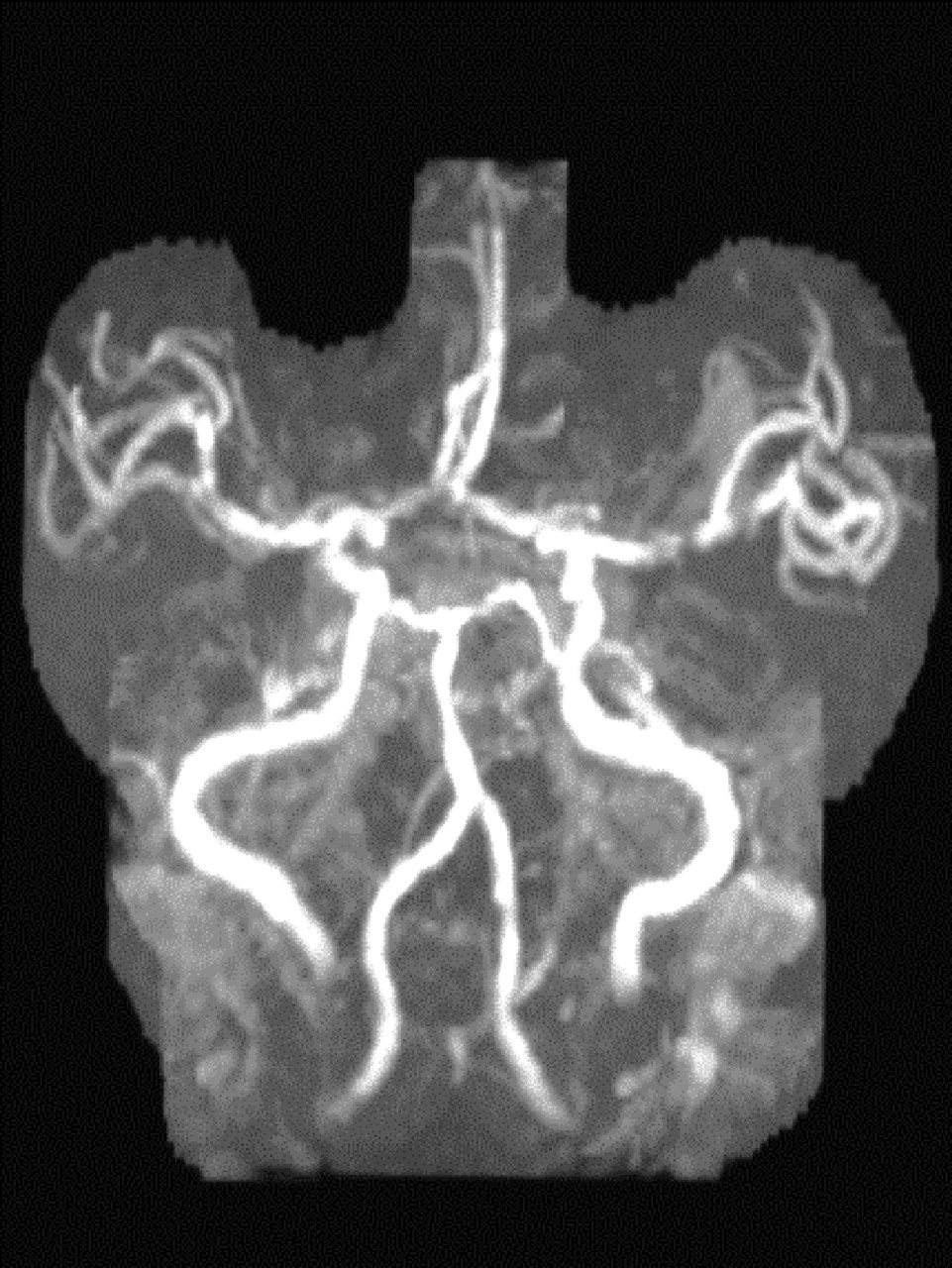
Our patient underwent both DWI and PWI scanning before and after administration of the tPA therapy. The initial DWI scan (Fig. 1) showed a hyperintense signal within the left lentiform nucleus (arrow). The initial PWI scan (Fig. 2) showed a larger, wedge-shaped area of delayed perfusion (outlined) involving most of the territory supplied by the middle cerebral artery (MCA). This finding was in keeping with a proximal MCA occlusion, as demonstrated on magnetic resonance angiography (Fig. 3, arrowhead).



Intravenous tPA therapy was started nearly 6 hours after the presumed onset of the stroke. One hour later some neurological improvement was observed, and 6 hours later the patient had some residual dysarthria, aphasia and facial weakness but had regained most of the strength in his right arm and leg and had a revised NIHSS score of 5. Although a repeat DWI scan at 6 hours post-tPA (Fig. 4) revealed changes in the left lentiform nucleus (arrow) that were similar to those seen before thrombolytic therapy, a repeat PWI scan showed reversal of many of the changes in the MCA-supplied territory (Fig. 5). The radiological improvement seen on the PWI scan and the neurological improvement seen clinically were in keeping with recanalization of the left MCA, as seen on magnetic resonance angiography (Fig. 6). CT scanning on subsequent days (not shown) confirmed the subcortical nature of the infarct, without hemorrhagic complication. After 48 hours the patient's NIHSS score had improved to 3, and he was referred for stroke rehabilitation before discharge home.

Although tPA is typically used only within the first 3 hours after onset of an acute ischemic stroke, a meta-analysis of thrombolytic studies has shown that patients may still benefit from tPA therapy if it is begun up to 6 hours after symptom onset, without a significant increase in the risk of hemorrhagic complications.2 The case we have described illustrates how MRI, of both perfusion and diffusion defects, may ultimately help to select patients who would benefit the most from tPA therapy in the 3–6-hour window.
Fintan O'Rourke N. Akhtar Derek Emery Ashfaq Shuaib Stroke Prevention Clinic Division of Neurology University of Alberta Hospital Edmonton, Alta.
References
In this issue

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Article tools






Jump to section
Related Articles
Cited By...
- No citing articles found.
More in this TOC Section
Similar Articles
Collections

