


- © 2004 Canadian Medical Association or its licensors
Abstract
Background: Physician decision-making and perceptions of patients are affected by a patient's socioeconomic status (SES). We sought to determine if the perceptions of first- and second-year medical students are similarly affected. We also wanted to determine whether a student's own SES affects his or her perceptions of patients from a low or high SES background.
Methods: Two similar videos of a physician–patient interview were created. One video featured a patient of apparently high SES and the other featured a patient of apparently low SES. Differences in SES were portrayed by means of clothing, accessories and dialogue. First- and second-year medical students at the University of Western Ontario were recruited to view 1 of the videos and to answer a questionnaire using a 5-point Likert scale.
Results: Responses were obtained from 205 (89%) of the 231 medical students invited to participate. Respondents' perceptions of the low SES and high SES patients were significantly different in the following respects. The low SES patient was perceived to be less compliant in taking medications and less likely to return for follow-up visits; was perceived to have a lower level of social support, poorer overall health and a worse prognosis; and was perceived to be more adversely affected in his occupational duties by illness (p < 0.05). Furthermore, second-year students who watched the video with the low SES patient were less inclined to want that patient in their practice than second-year students who watched the video with the high SES patient (p = 0.032). One hundred and six students (52%) were categorized as having high SES and 37 (18%) as having low SES (the remaining students were categorized as having mid-level SES). Among students who watched the video with the low SES patient, the level of agreement with the statement “This person is the kind of patient I would like to have in my practice” was greater among low SES students than among high SES students (p = 0.012).
Interpretation: First- and second-year medical students have negative perceptions of low SES patients on several dimensions.
In spite of the fact that Canada has a universal and accessible health care system, Canadians experience disparities in the delivery of health care according to their income level.1,2,3,4Physicians' perceptions of their patients can be influenced by the patients' socioeconomic status (SES), and in turn these perceptions affect the health care that the physicians provide.5,6 Previous studies have emphasized the need to understand the origins of such perceptions. Using a video portraying a typical physician–patient interview and a survey administered to first- and second-year medical students, we examined students' perceptions of patients from different socioeconomic backgrounds. Our hypothesis was that medical students would have negative perceptions of low SES patients. Furthermore, we wished to determine whether any differences in perception existed between first- and second-year medical students and between students with low and high SES.
Methods
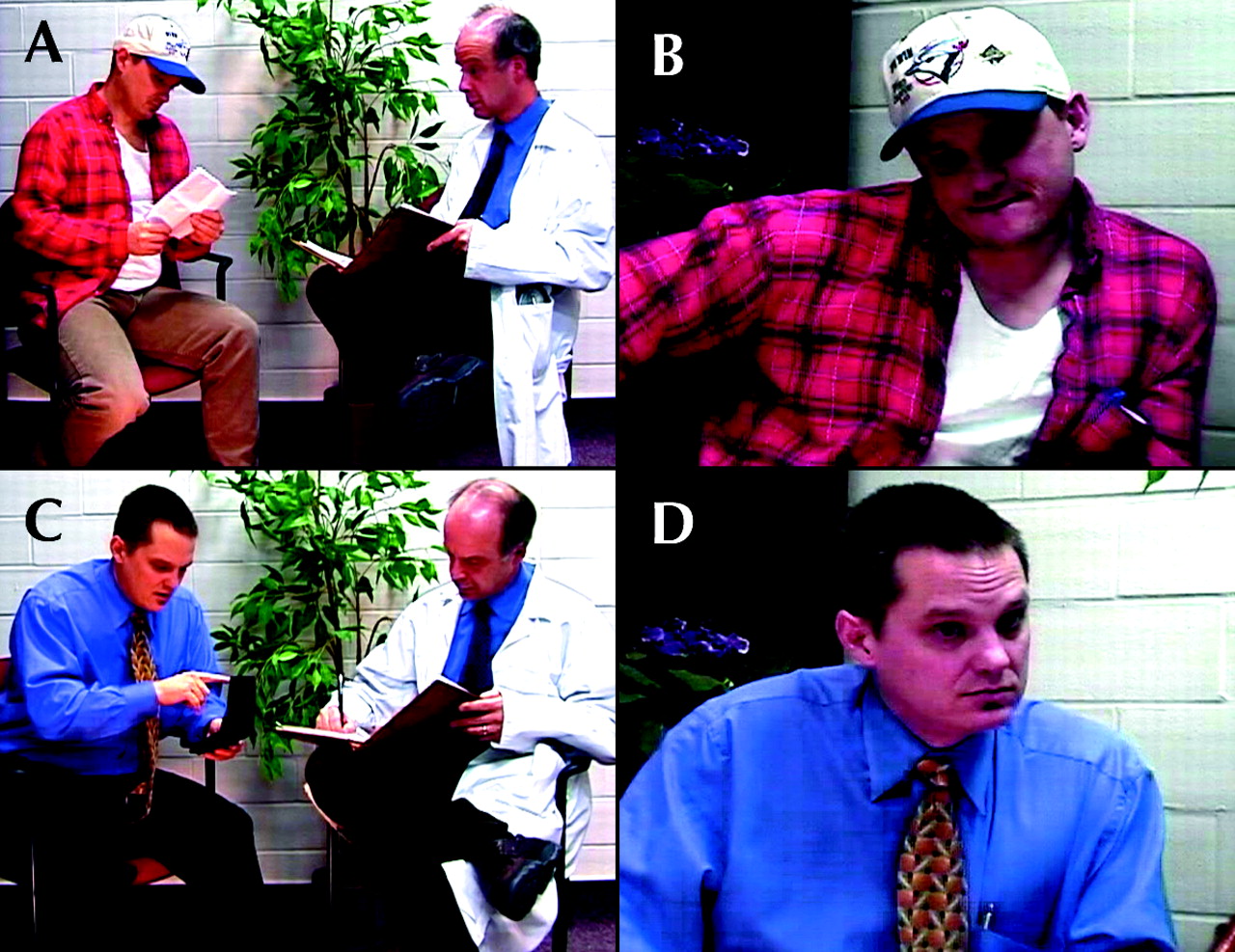
Two videos depicting a physician–patient interview, one with a low SES patient and the other with a high SES patient, were filmed. The roles of physician and patient were played by 2 professional male actors hired by the University of Western Ontario (UWO) Standardized Patient Program. One actor played the role of the physician in both videos, and the other actor played the roles of both the low SES patient and the high SES patient. The scripts in the 2 videos were similar, differing only in terms of some of the patient responses (Box 1). Differences in the patients' apparent SES were shown through clothing, hygiene, accessories, language and script (Fig. 1, Table 1). The videos can be viewed online at www.cmaj.ca/cgi/content/full/170/13/1915/DC1.
Table 1.

Fig. 1: (a) Still from the video with the patient of low socioeconomic status (SES), showing both patient and physician; (b) close-up of low SES patient; (c) still from the video with the high SES patient, showing both patient and physician; (d) close-up of high SES patient.

With the help of 6 other students, we developed a survey that used bipolar 5-point Likert rating scales to capture student responses, with 1 representing the negative extreme (e.g., noncompliant) and 5 representing the positive extreme (e.g., extremely compliant). Ethics approval was obtained from the UWO Research Ethics Board.
First- and second-year UWO medical students were recruited for and participated in the study on Apr. 9 and 14, 2003, respectively, during patient-centred learning (PCL) course time. Each PCL group of 8 students was predetermined before the study by the Undergraduate Medical Education (UME) office. Assignment to PCL groups was not completely random: the UME office attempted to ensure approximately equal numbers of male and female students in each PCL group. Students in even-numbered PCL groups viewed the video with the low SES patient and those in odd-numbered PCL groups viewed the video with the high SES patient. No incentives were given to students, participation in the study was voluntary and informed consent was obtained. Students were not aware that perceptions of patient SES were being measured. After presentation of the video, each student completed the survey. Students were asked to keep their knowledge of the study confidential until Apr. 15, 2003.
Two-sample independent t tests were used to compare responses between students who viewed the low SES video and those who viewed the high SES video (within each medical school year). Surveys were also grouped according to students' self-reported gross family income, with low SES defined as family income less than $61 000 and high SES defined as family income greater than $100 999; students with a self-reported gross family income between $61 000 and $100 999 were excluded from this particular analysis. The responses of low and high SES students were compared with 2-sample independent t tests for each video.
Results
Responses were obtained from 205 (89%) of the 231 medical students invited to participate. Of these, 48 (23% of the total) and 58 (28%) first-year students watched the high and low SES videos respectively, while 52 (25%) and 47 (23%) second-year students watched the high and low SES videos respectively. Student characteristics are presented in Table 2. Although no significant difference in gross family income was detected for first-year students, first-year students who watched the high SES video considered themselves to be of a higher socioeconomic class than those who watched the low SES video (p = 0.042). First-year students who watched the low SES video were significantly older (by a mean of 8 months) than first-year students who watched the high SES video (p = 0.015).
Table 2.
Both first- and second-year students perceived that the low SES patient would be less compliant in taking his medications (p < 0.001 and p = 0.001 respectively), would be less likely to come in for monthly follow-up (p = 0.004 and p = 0.033 respectively) and would have a lower level of social support (p < 0.001 for both groups) than the high SES patient (Table 3). Among both first- and second-year students, there was no significant difference between those who watched the low SES video and those who watched the high SES video in perception of the patient's truthfulness about his drinking habits. Students in both years identified the patient in the low SES video as having low SES and the patient in the high SES video as having high SES (p < 0.001), which confirmed that a difference in SES was apparent.
Table 3.
With further analysis, 106 (52%) and 37 (18%) surveys were categorized as representing responses of high and low SES students respectively (data not shown). Low SES students perceived that the high SES patient was less likely to come in for a monthly follow-up (p = 0.049). Among students who watched the video with the low SES patient, the level of agreement with the statement “This person is the kind of patient I would like to have in my practice” was greater among low SES students than among high SES students (p = 0.012).
Interpretation
To our knowledge, medical students' perceptions of high and low SES patients have not been evaluated in any substantial published study. Our results support the hypothesis that medical students have negative perceptions of low SES patients. The low SES patient was perceived to be less compliant; to have less social support, poorer overall health and a poorer prognosis; and to be more adversely affected with respect to his occupational duties than the high SES patient. Furthermore, second-year students and high SES students showed a greater preference to have the high SES patient in their practice rather than the low SES patient. Overall, second-year students had negative perceptions of low SES patients on a greater number of dimensions than first-year students.
These medical students' perceptions mirror some of the perceptions that other investigators have found among physicians. For example, van Ryn and Burke6 demonstrated that physicians are more likely to perceive low SES patients as being less intelligent, independent, responsible, rational, physically active and compliant and as having less significant career demands than high SES patients. In a study of general practitioner decision-making, Scott and associates5 found that diagnostic tests were less likely to be ordered for low SES patients than for high SES patients and that low SES patients were more likely to receive a prescription. However, patient SES was not associated with a physician's decision to follow up. In our study of medical students, patient SES was not significantly associated with the decision to refer to a specialist.
The parental income of the UWO first- and second-year classes was similar to that of other Canadian medical school classes,7 in that students from high-income families were overrepresented and students from low-income families were underrepresented. Our results suggest that low SES students would prefer low SES patients in their practices more than high SES students would. This finding complements previous work characterizing US physicians who provide high levels of service to underserved populations.8 Physicians with low SES backgrounds (low parental income and education) showed significantly higher levels of service to poor patients than physicians with high SES backgrounds, even after adjustment for physician race, ethnic background and sex.
The cause of negative perceptions of low SES patients is unclear. For example, although some studies suggest that lower SES is an independent risk factor for lower compliance and follow-up attendance,9,10,11,12 others have found either no correlation13,14 or greater compliance among low SES patients.15 Socioeconomic factors are associated with true patient differences in certain cases. For instance, physicians perceive low SES patients as being less likely to desire a very physically active lifestyle, a perception that is consistent with research findings.6,16,17,18 However, if a physician applies such an epidemiologically supported, population-based likelihood to an individual patient, without regard for any contradicting evidence for that patient, then the stereotype is not deserved.
Several limitations of this study should be considered. First-year students watching the low SES video were significantly older than those watching the high SES video. The scripts for the 2 videos were similar, but the personality and behavioural mannerisms of the patient varied slightly between videos, which might have had an effect on student responses. The lack of an option such as “There isn't enough information to answer the question” meant that students who wanted more information were forced to choose a response on the 5-point Likert scale that might not have reflected their opinion accurately. Our study was not longitudinal, so any differences between first- and second-year students might have been due to differences in the sample itself, rather than to differences between years of education. The differences detected were subtle (none exceeded 1.0 on the Likert scale) and might not have been clinically significant. Perceptions could vary from encounter to encounter but each student viewed only 1 video; thus, it might be necessary to have subjects view more cases to achieve a more realistic understanding of perceptual differences. First- and second-year medical students do not have a great deal of contact with patients, so their perceptions are not yet shaped by real-world experience. The generalizability of this study may be limited because subjects consisted of UWO medical students only. Finally, the arbitrary low- income cutoff of $60 999 would probably not be perceived as a low income by the average Canadian family.
Our results demonstrate that medical students have negative perceptions of low SES patients. More negative perceptions were found among second-year students, but the reason for this difference is unclear. Low SES students had a greater willingness than high SES students to have the low SES patient in their future practice. We have expanded on earlier studies by demonstrating that physicians' negative perceptions of low SES patients are apparent at an early stage in their training. Delineating the origins of these perceptions is an important avenue of research that needs to be explored.
𝛃 See related article page 1920
Footnotes
-
This article has been peer reviewed.
Contributors: James Woo and Cheong Lee were equally responsible for conceiving the project. James Woo was responsible for coordinating the project. All authors shared the work of collecting and analyzing the data and writing the manuscript.
Acknowledgements: We are grateful to Nina Ghosh, Dmitry Guller, David Huxley, Anna Labuda and Ali Namazie for their assistance in creating the videos and developing and administering the survey, to Judy McCormick and the University of Western Ontario Standardized Patient Program for their support in production of the videos, to Dr. Peter Flanagan for reviewing our proposal and manuscript, to Dr. Jeffrey Nisker for reviewing our proposal, and to Dr. Jacalyn Duffin and Dr. Milton Woo for critically reviewing our manuscript.
Competing interests: None declared.
Correspondence to: James Woo, 87 Nanette Dr., London ON N5X 3L3; jwoo4uwo.ca
References
In this issue

{kind=link}
{kind=link}
Article tools






Jump to section
Related Articles
Cited By...
- Six Recommendations for Provider Behavior Change in Family Planning
- Health professionals implicit bias of adult patients with low socioeconomic status (SES) and its effects on clinical decision-making: a scoping review protocol
- Students' Comfort Level in Treating Vulnerable Populations and Future Willingness to Treat: Results Prior to Extramural Participation
More in this TOC Section
Similar Articles

