


Background and epidemiology: Speech is a remarkable and complicated achievement involving a variety of linguistic, cognitive and sensorimotor processes. Little wonder that about 85% of children between the ages of 2 and 6 encounter a few bumps and breaks along the path to fluent speech.1 Preschool children normally go through a period of dysfluency; about 10% of preschoolers experience a speech or language delay or disorder serious enough to benefit from early referral and assessment by a speech-language pathologist (SLP). The etiology and mechanisms of developmental speech dysfluency are complicated and a matter of some debate. In general, it signals a lack of coordination between linguistic intention and motor articulation as children learn to talk and think at the same time.
Common examples of developmental dysfluency include repetitions, interjections, pauses, revisions and mistiming (Box 1). Children may repeat individual sounds or syllables, especially at the beginning of words. Interjections are extra sounds, syllables or words that add no meaning to the message. Pauses or blocking (silent intervals between or within words), may be considered a type of dysfluency, especially when they last more than 2 seconds. Revision refers to the habit of stopping in midstream and starting over in a new direction. Mistiming refers to the prolongation of sounds or syllables.1

Most children outgrow the period of dysfluency, but those who do not will require speech therapy, so it is important that a distinction be made between childhood dysfluency and stuttering. Stuttering is a disturbance in the normal fluency and time patterning of speech that is inappropriate for the person's age. We all experience periods of dysfluency — normal speech includes 2%–4% interruptions in flow or fluency. Generally speaking, revisions, interjections and word and phrase repetitions are very common in children's speech; sound and syllable repetition, sound prolongation and broken words are more atypical.
Speech patterns and behaviours that might signal that a child is at risk of stuttering include within-word or part-word repetitions, prolonged sounds, avoiding speaking situations or saying “I can't say it,” looking upset, speaking with tension in the face or neck muscles or voice and speaking with unexpected rises in pitch or loudness.1 Boys are 4 times more likely than girls to develop a stutter. Children with a family history of stuttering are more likely to stutter than children without.
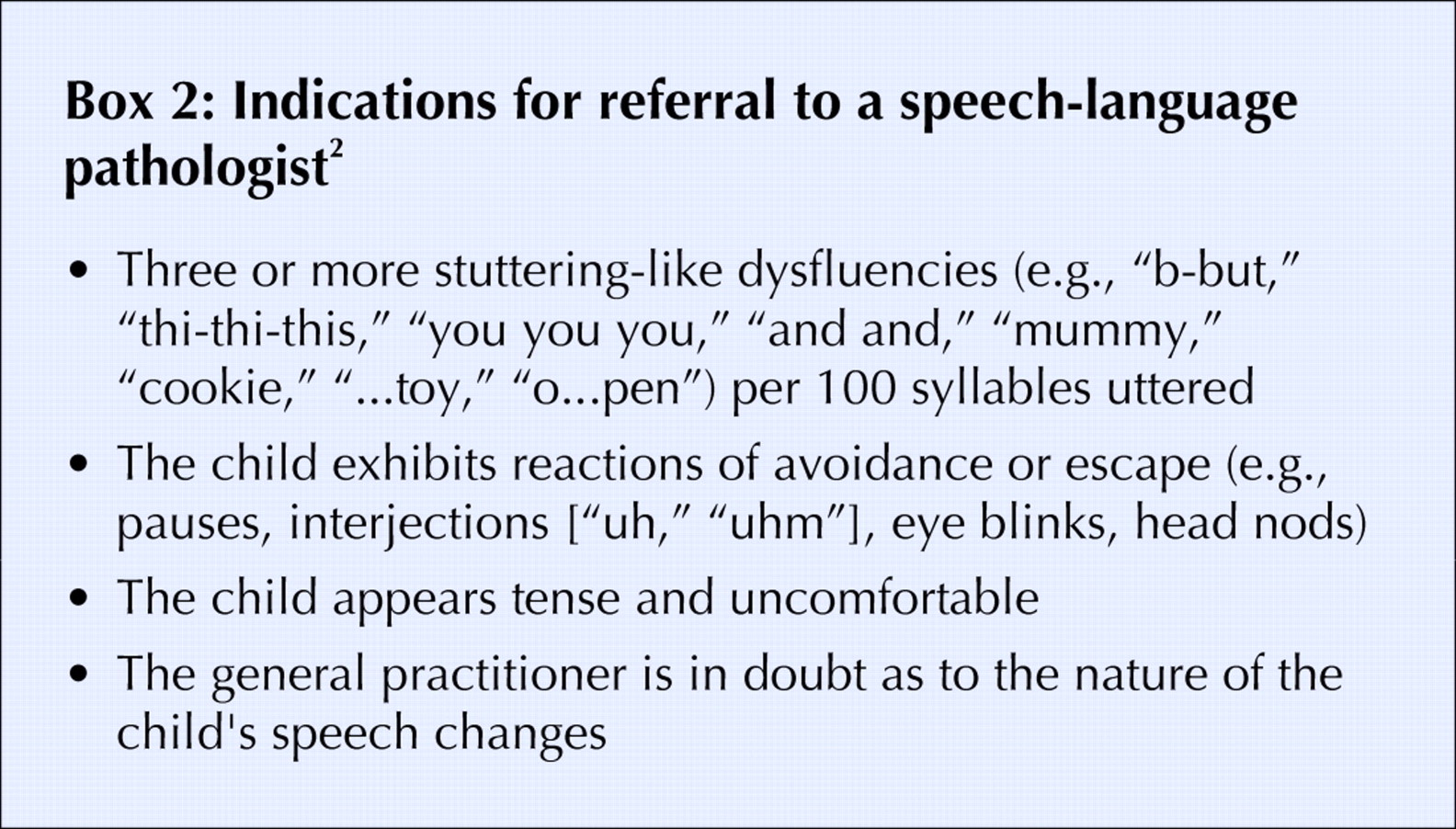
Clinical management: In general, primary care physicians can reassure parents that transient speech dysfluency is normal in preschoolers. However, they also need to be aware of the indications for referral of children to an SLP2 (Box 2). Parents know their child the best, so lingering parental concern may be reason enough to refer the child for speech and language assessment. A physician referral to an SLP is not usually required in most provinces, but physicians can refer with a parent's consent.
The SLP evaluates the child and then makes appropriate recommendations based on each child and their family according to factors such as severity of disorder, type and frequency of dysfluencies, parental commitment and concomitant developmental delays. For preschool fluency, the first therapeutic step usually involves training the parent to facilitate a more fluent speech environment in day-to-day interactions. The SLP may also provide a home program or monitor the child's progress regularly. Therapy could occur in a parent education group or in a group with several children and families.
SLPs must complete a minimum of a master's degree in Speech-Language Pathology in order to practise in Canada. These specialists are in short supply and high demand, so early referral is optimal. In general, preschool and school-based speech and language services are government-funded. Most private insurance plans will offer some coverage, under rehabilitative services.
Prevention: The etiology of stuttering is not completely understood. Adults can mitigate the risk of stuttering by reducing the conversational demands on a child — that is, by assuming a “Mr. Rogers” approach to conversation by modeling slow, smooth speech, acknowledging when speech is difficult and creating special talk time (Box 3).

Erica Weir Associate Medical Officer of Health Sonya Bianchet Speech-Language Pathologist Early Expressions Speech and Language Services Kingston, Frontenac and Lennox & Addington Health Unit Kingston, Ont.
Footnotes
-
For more information consult the Canadian Association of Speech-Language Pathologists and Audiologists: www.caslpa.ca.
References
In this issue

{kind=link}
{kind=link}
{kind=link}
Article tools






Jump to section
Related Articles
Cited By...
More in this TOC Section
Similar Articles
Collections

