


Abstract
FACTOR V LEIDEN IS A COMMON GENETIC MUTATION that predisposes its carriers to venous thromboembolism. When combined with the hypercoagulable state that is characteristic of pregnancy, there is an increased risk of severe and recurrent pregnancy complications. Factor V Leiden is the most common cause of primary and recurrent venous thromboembolism in pregnancy. Factor V Leiden carriage has consistently been shown to increase the risk of early onset gestational hypertension and HELLP syndrome (Hemolysis, Elevated Liver enzymes, Low Platelets) in pregnancy. Maternal carriage of factor V Leiden is also associated with severe placental abruption and fetal growth disturbances. Although it is unclear whether factor V Leiden causes an increased risk of first trimester miscarriage, it is associated with stillbirth and placental infarction. Patients with venous thromboembolism or severe pregnancy complications should be tested for factor V Leiden and other inherited and acquired thrombophilia. Therapeutic heparin is required for acute thromboembolic events in pregnancy. Patients with factor V Leiden and a previous venous thromboembolism may, according to their level of risk, be offered either prophylactic or therapeutic heparin. The role of antithrombotic therapy in the prevention of severe pregnancy complications remains unclear.
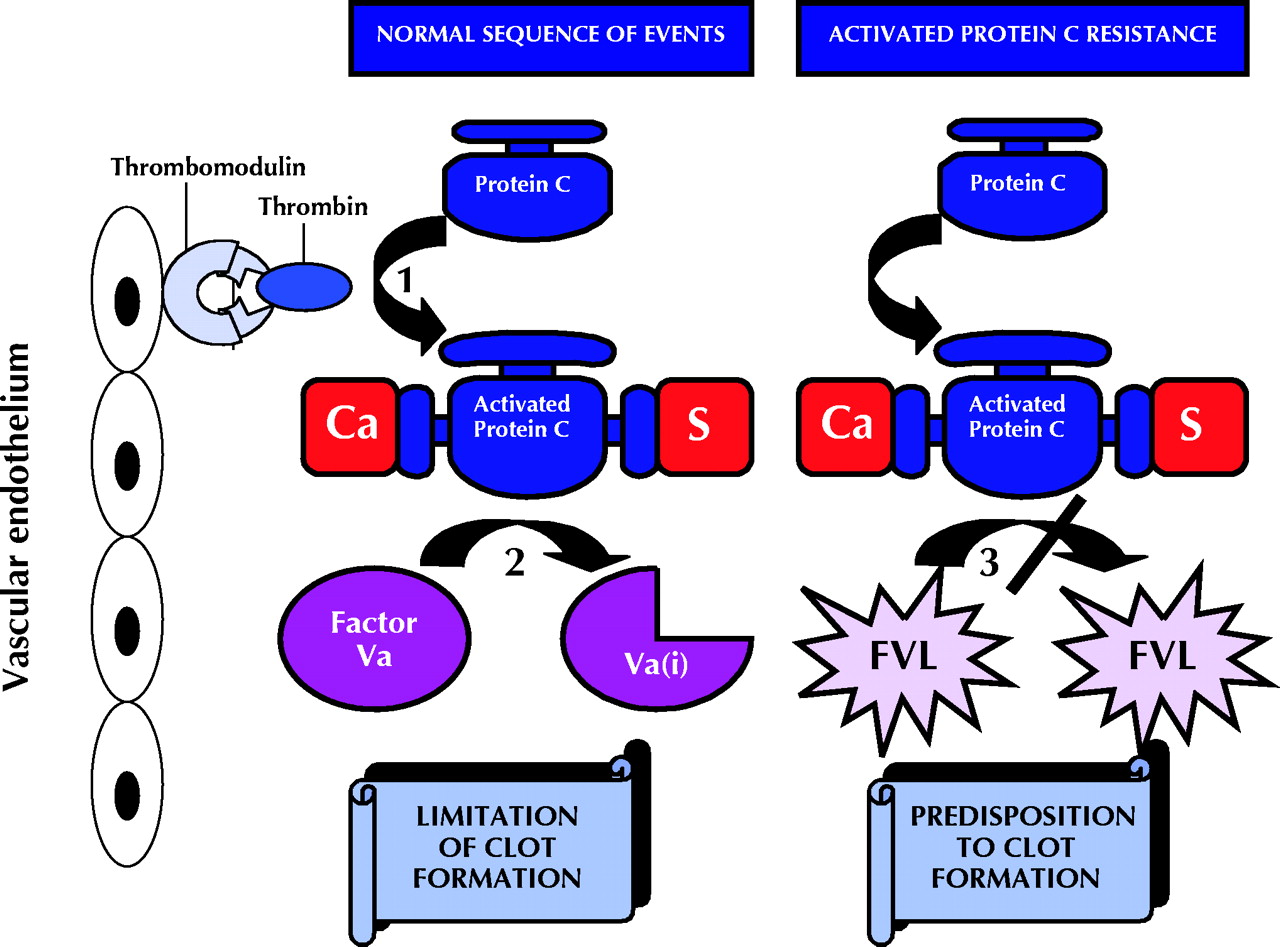
The term thrombophilia refers to familial or acquired hemostatic disorders that result in a predisposition to thromboembolic events.1 Inherited activated protein C resistance is the most frequent genetic cause of venous thrombosis.2 The factor V Leiden mutation is responsible for 95% of cases of activated protein C resistance.3 Activated protein C is a naturally occurring anticoagulant that is essential to the balance of procoagulant and anticoagulant mechanisms in the circulation.4 Protein C is activated by the binding of the thrombin–thrombomodulin complex onto endothelial cells. In the presence of protein S, another natural anticoagulant and cofactor to protein C, activated protein C selectively degrades coagulation factors Va and VIIIa.3 This results in the limitation of clot formation. The factor V Leiden mutation is caused by a point mutation in the factor V gene, encoding a substitution of arginine for glutamine at position 506 of the factor V molecule, the site at which activated protein C cleaves factor Va.3 The factor V Leiden mutation renders factor Va resistant to the anticoagulant effects of activated protein C, resulting in a genetic predisposition to thrombosis (Fig. 1).3

Fig. 1: Activated protein C anticoagulant pathway: 1. Thrombin binds to an endothelial cell receptor, thrombomodulin, and becomes an anticoagulant protein capable of activating protein C. 2. In the presence of protein S (S) and ionized calcium (Ca), activated protein C inactivates coagulation factors Va and VIIIa. Only factors Va and inactivated Va(i) are shown here. This is the mechanism whereby clot formation is limited. 3. Factor V Leiden (FVL) is a mutation in the factor V molecule, rendering it resistant to cleavage by activated protein C. Factor V remains a procoagulant and thus predisposes the carrier to clot formation.
The Leiden mutation is reported in 5% of the healthy white population,5 1% of the healthy black population5 and 3% of low-risk obstetric patients.6 In individuals with a personal or family history of thrombosis, carrier rates range from 20% to 60%.3 Heterozygosity for the factor V mutation is associated with a 5–10-fold increase in the risk of thrombosis, whereas homozygosity confers a 50–100-fold increase in risk.2,7
Diagnosis of factor V Leiden in pregnancy
The factor V Leiden mutation is detected readily and accurately with molecular DNA techniques.7 Genomic DNA may be extracted and the polymerase chain reaction (PCR) used to amplify exon 10 of the factor V gene. This 267 base pair gene segment contains nucleotide 1691, which is where the most common mutation occurs. The amplified product is then subjected to enzymatic degradation and fractionated by size on a polyacrylamide gel.3 The patient is then classified as a noncarrier, heterozygous or homozygous depending on whether no copies, one copy or 2 copies respectively of the factor V Leiden mutation are detected.8
An increased incidence of factor V Leiden carriage has been reported in women who have experienced previous severe complications of pregnancy.9,10,11 Twenty percent of women with a history of placental abruption, fetal death, severe pre-eclampsia or intrauterine growth restriction were found to be carriers of the mutation compared with 6% of women with uncomplicated pregnancies (odds ratio 3.7; p = 0.003).10 The greater the number of previous adverse outcomes, the higher the likelihood of a thrombophilia being present.11 Even in the absence of a previous thromboembolism, women with severe pregnancy complications should be tested for inherited and acquired thrombophilias.10,12
Maternal complications
Venous thrombosis
Normal pregnancy is accompanied by changes in the coagulation and fibrinolytic systems. These include an increase in a number of clotting factors (I, II, VII, VIII, IX and XII), a decrease in protein S levels and inhibition of fibrinolysis.12,13,14,15 There is also a significant fall in the activity of activated protein C, an important anticoagulant, as gestation progresses.16 These physiologic changes may be important to minimize intrapartum blood loss but confer an increased risk of thromboembolism during pregnancy and the postpartum period.12 Hyperestrogenism, either from pregnancy or oral contraceptives, is the most frequent cofactor associated with congenital thrombophilias.2,17,18,19
Venous thromboembolism occurs in one in 1500 pregnancies18,20 and is the leading cause of morbidity and mortality in pregnancy and the postpartum period.6,21,22 Up to one-quarter of untreated deep vein thromboses in pregnancy progress to a pulmonary embolus, which is associated with a 12%–15% mortality rate.6,21 Women with a history of venous thromboembolism during pregnancy or the puerperium have a higher prevalence of factor V Leiden carriage than women with no such history.6,13,14,19,20,23,24 The reported incidence of factor V Leiden carriage in published series varies from 13% to 78%,6,13,14,19,20,24 with relative risks between 5 and 16.14,19,20 The largest published study reports the prevalence of factor V Leiden to be 44% among 119 women with a history of pregnancy-related venous thromboembolism compared with a rate of 7.7% among 233 age-matched women (relative risk 15.2).20
Hypertensive disorders of pregnancy
The available evidence suggests a 2–6-fold increase in the risk of pre-eclampsia in women carrying the factor V Leiden mutation.25,26,27,28,29,30 Dizon-Townson and colleagues found heterozygous factor V Leiden in 8.9% of women with severe pre-eclampsia compared with 4.2% of normotensive controls.25 Likewise, Grandone and coworkers reported a 10.5% prevalence of the mutation in 96 women with pre-eclampsia compared with 2.3% of 129 healthy controls (odds ratio 4.9, 95% confidence interval [CI] 1.3–18.3).27 Higher values were reported in a recent study in which 18% of 120 women with pre-eclampsia carried the factor V mutation compared with only 3% of healthy controls (relative risk 6.17, 95% CI 1.9–20; p < 0.001 ).30 A similar association between factor V Leiden carriage and HELLP syndrome (Hemolysis, Elevated Liver enzymes, Low Platelets) has been reported.29,30,31 The central mechanism in these disease processes is thought to be endothelial cell injury and dysfunction from fibrin deposition and microthrombi formation induced by the maternal hypercoagulable state.25,29
Fetal complications
Pregnancy loss
The association between maternal factor V Leiden carriage and first trimester miscarriage is in dispute. A large retrospective cohort study that investigated the reproductive histories of 228 carriers of factor V Leiden and 121 noncarrier controls found that carriers had over twice the risk of fetal loss overall, particularly early losses. In this study, 80% of losses occurred within the first 16 weeks of pregnancy.32 However, the largest prospective cohort study that examined over 1500 pregnancies affected by maternal thrombophilia did not find a statistically significant increase in first trimester miscarriage.33 Similarly, a recent abstract describing 376 patients with previous pregnancy losses found no association between recurrent first trimester loss and maternal thrombophilia, and challenged the increasing use of anticoagulant therapy in these patients.34
The association between maternal carriage of factor V Leiden and late fetal losses or stillbirths is more consistent.10,33,35,36,37,38,39 Some 20%–50% of women who had late pregnancy losses were reported to carry factor V Leiden compared with less than 5% of parous women with no history of pregnancy loss.35,36,37,38,39 Thrombophilia carriers are 3–5 times more likely to have a stillbirth than noncarriers,33,39 with this risk rising steeply in the presence of multiple thrombophilic defects.33 In many cases, placental evidence of thrombosis and infarction accompanied the intrauterine death.37,38
Abruption
Some 25%–50% of patients with a previous history of placental abruption reportedly carry factor V Leiden.10,40,41 In a retrospective cohort study that examined pregnancies with poor outcome, 57% of patients with placental abruption were found to be thrombophilia carriers compared with 22% of controls (p = 0.005).34
Intrauterine growth restriction
The association between factor V Leiden and intrauterine growth restriction was first reported in a case series describing 5 of 7 patients with severe and recurrent intrauterine growth restriction who carried the mutation.9 Patients with intrauterine growth restriction were considered to be a subgroup in a case–control study that examined 110 women with obstetric complications compared with 110 controls with uncomplicated pregnancies. Five of 22 patients with severe intrauterine growth restriction carried factor V Leiden (odds ratio 1.9, 95% CI 0.6–6.3), after exclusion of other causes of fetal growth disturbances.10 Likewise, in a retrospective review considering 377 pregnancies with a poor outcome, maternal thrombophilia was found in over 50% of pregnancies complicated by intrauterine growth restriction compared with 24% in normal, uncomplicated pregnancies (p = 0.007).11 Lee describes how 6 of 23 women with severe intrauterine growth restriction were found to be heterozygous for the factor V Leiden or prothrombin gene mutation compared with no patients in the control group.42 Other studies have failed to confirm these findings.18,30,43,44
Treatment options for maternal thrombophilia carriage
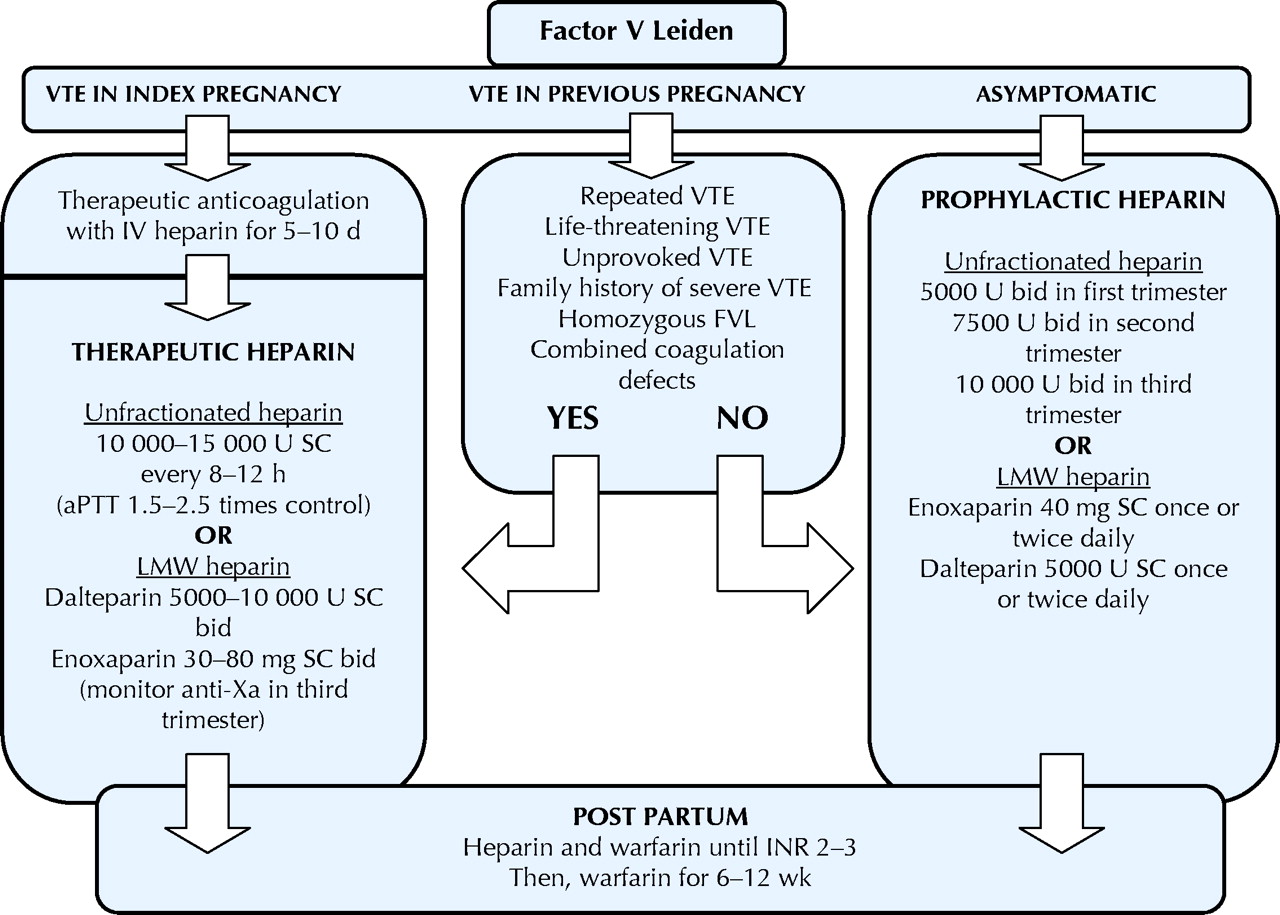
There have been no randomized controlled trials of treatment for patients known to be carrying the factor V Leiden mutation.8 It is also unknown whether prophylactic treatment of asymptomatic carriers or of carriers with a previous poor obstetric outcome is effective. The following is a summary of published documents outlining expert opinion and possible management strategies (Fig. 2).45,46
{kind=link}
{kind=link}
Fig. 2: Treatment of thromboembolic complications associated with factor V Leiden carriage in pregnancy. VTE = venous thromboembolism, IV = intravenous, SC = subcutaneously, aPTT = activated partial thromboplastin time, LMW = low-molecular-weight, bid = twice a day, FVL = factor V Leiden, INR = international normalizing ratio.
1. Acute thromboembolic event in index pregnancy (first event)
Patients with or without a coagulopathy who develop an acute thromboembolism during pregnancy require full anticoagulation with intravenous unfractionated heparin for 5–10 days.46,47,48,49 An intravenous bolus of heparin followed by a continuous infusion aimed at maintaining the activated partial thromboplastin time (aPTT) at 1.5–2.5 times the control value is recommended.45,46,47,50 Patients may then be converted to subcutaneous unfractionated heparin,45,47 administered every 8–12 hours, titrating to an aPTT obtained 6 hours after injection of 1.5–2.5 times the control value.48,49 This requires doses of about 10 000–15 000 U each.49 Changes in heparin metabolism during pregnancy may shorten its half-life, requiring increasing dosages with advancing gestation.47 Although some recommend full anticoagulation for the remainder of the pregnancy,45,50 other experts suggest a decreased dose after 1–3 months of full anticoagulation to limit the risk of osteoporosis.46,48 The severity and underlying cause of the thrombotic episode may be used to help tailor this decision to the individual patient.46 Heparin should be discontinued immediately before delivery, and then both heparin and warfarin can be started post partum. Once a therapeutic international normalizing ratio of 2–3 is obtained, heparin can be discontinued and warfarin continued for 6–12 weeks post partum.45,47,48,50
Alternatively, because of the significant advantages of low molecular weight (LMW) heparin, many suggest that it should be an alternative after the initial 5–10-day period of intravenous unfractionated heparin.46,48,50 This involves subcutaneous administration twice daily during pregnancy to achieve therapeutic levels.46,50 The safety and efficacy of LMW heparin for initial treatment of venous thromboembolism have been demonstrated in the nonpregnant state,51 and it is an acceptable alternative to unfractionated heparin.15 Doses similar to those used in the nonpregnant state are suggested, with monitoring of the anti-Xa level advised.15 Consensus is lacking concerning the frequency of monitoring of anti-Xa levels, with recommendations ranging from periodic monitoring,48 to a single third trimester level,50 to testing peak anti-Xa activity during the first month of use and monthly thereafter.46
Long-term anticoagulation for individuals with inherited thrombophilia may be considered after one thromboembolic event12,50 and recommended after 2 or more thromboembolic events.1 This is especially relevant if the initial acute event was life threatening52 or if there is a family history of fatal venous thromboembolism.12
2. Factor V Leiden and previous venous thromboembolism
Considerable controversy exists concerning which patients should receive thromboprophylaxis in pregnancy and the dosages of heparin that should be used. Although it is unclear whether thromboprophylaxis is necessary or effective in healthy women with one previous venous thromboembolism,50 most authors suggest thromboprophylaxis for patients with a previous venous thromboembolism and a known thrombophilia.45,47,48,53,54
Patients who are already on long-term anticoagulation should continue full anticoagulation throughout pregnancy and for 6–12 weeks post partum.45,50 This may be achieved with adjusted doses of standard heparin or LMW heparin as soon as pregnancy is confirmed.12,55 Heparin may be started while attempting to conceive, or upon first diagnosis of pregnancy, in an effort to avoid fetal exposure to warfarin.1 The greatest risk of warfarin-induced embryopathy occurs with exposure at 6–12 weeks' gestation.1 Oral anticoagulants are safe for breast-feeding women and may be started post partum53
For those women not on long-term anticoagulation who have had one previous venous thromboembolism and a diagnosed thrombophilia, treatment options include prophylactic heparin8,47,49 or adjusted-dose (therapeutic) heparin1,45,52 during pregnancy, and oral anticoagulation for 6 weeks post partum.1,50 A common prophylactic regimen consists of unfractionated heparin, 5000 U every 12 hours in the first trimester, 7500 U every 12 hours in the second trimester and 10 000 U every 12 hours in the third trimester.47,48 Alternatively, LMW heparin may be administered once49,54 or twice daily.48 Suggested prophylactic regimens include dalteparin, 5000 U, or enoxaparin,40 mg once or twice daily.48,55 LMW heparin has been used successfully during pregnancy in 486 patients in 21 studies of thrombophilia and can be considered effective, safe and convenient prophylaxis for thrombophilia in pregnancy.55,56
The lack of prospective and randomized studies to dictate management has led some to employ an approach of patient risk stratification based on details of the individual case history.1,53 High-risk patients are those with repeated thromboembolic events, events that are life threatening and events that are unprovoked.1,45,53 Patients with these features, in addition to those with a family history of serious thromboembolic complications, are deemed to be at higher risk for recurrent events.1,45,52 Patients with homozygous factor V Leiden and combined coagulation defects are also at significant risk of recurrence, warranting more aggressive thromboprophylaxis.8,48,53 A synergistic interaction occurs with carriage of more than one thrombophilic defect, placing these patients at an exponentially increased risk of a thromboembolic event.57,58,59 In the absence of these high-risk features, the risk of recurrent venous thromboembolism may be less than previously thought. A recent prospective study reported the risk of recurrent venous thromboembolism in the absence of antepartum prophylaxis to be only 2.4% in those with no thrombophilia and 5.9% in those with a thrombophilia.60
3. Factor V Leiden and previous pregnancy complication
No randomized prospective studies have been published that examine the efficacy of antithrombotic therapy in women with previous obstetric complications. Existing reports are retrospective and lack the appropriate control groups and patient numbers. Although many of these patients are treated with prophylactic heparin in subsequent pregnancies,49 the effectiveness of this treatment is unknown.
In a recent nonrandomized prospective study, prophylaxis with LMW heparin was reported to reduce fetal loss, with a success rate of 93% in the prevention group compared with 80% in the nontreated placebo group.61 Likewise, Hoffmann and colleagues observed a live birth rate of 69% after treatment with enoxaparin, 40 mg/day, compared with a rate of 83% in women treated with enoxaparin, 80 mg/day, and 20% in an untreated control group.62 Multicentre randomized controlled trials will be required to establish the efficacy of antithrombotic therapy in improving fetal health.
4. Factor V Leiden with no previous venous thromboembolism or pregnancy complication
It is not known whether patients with factor V Leiden, but without a previous history of thrombosis or adverse pregnancy outcome, need thromboprophylaxis during pregnancy or the postpartum period.49 Most authors recommend low-dose prophylactic heparin throughout pregnancy followed by oral anticoagulation for 6–12 weeks post partum.12,45,48,49,52 Alternatively, LMW heparin or oral anticoagulants may be employed in the postpartum period only,53,54 because it appears to be the time of highest risk for patients with inherited protein deficiencies.52,63 Many European clinicians consider heterozygous factor V Leiden with no previous venous thromboembolism or pregnancy complications to be the thrombophilia with the lowest thrombotic risk and suggest clinical surveillance alone.46
Screening for factor V Leiden
At present, screening for inherited or acquired thrombophilias is best limited to women with a personal or family history of venous thrombosis, early onset or recurrent pre-eclampsia, recurrent fetal growth restriction, unexplained fetal loss or stillbirth, and placental abruption.12,48,49 The financial and personal costs associated with implementation of thrombophilia screening for severe pregnancy complications are unknown. The role of anticoagulant therapy in preventing future pregnancy complications needs to be investigated using a randomized controlled trial.
Conclusion
Factor V Leiden is a common gene mutation, which results in a genetic predisposition to thromboembolic complications. When combined with the prothrombotic influences of pregnancy, women who are carriers of factor V Leiden are faced with an increased risk of stillbirth, early onset pre-eclampsia, severe abruption and possibly fetal growth restriction. It is unclear whether heparin therapy reduces these pregnancy complications or improves pregnancy outcome. Women with factor V Leiden and a personal or family history of thrombosis probably benefit from thromboprophylaxis in pregnancy.
Footnotes
-
This article has been peer reviewed.
Contributors: Dena Bloomenthal acquired and organized the information, drafted the article and revised the article using the ideas and contributions of each author. Peter von Dadelszen, Robert Liston, Laura Magee and Peter Tsang critically revised the article for intellectual content, contributed to the analysis and interpretation of data, and gave final approval of the version to be published.
Competing interests: None declared.
References
- 1.↵
- 2.↵
- 3.↵
- 4.↵
- 5.↵
- 6.↵
- 7.↵
- 8.↵
- 9.↵
- 10.↵
- 11.↵
- 12.↵
- 13.↵
- 14.↵
- 15.↵
- 16.↵
- 17.↵
- 18.↵
- 19.↵
- 20.↵
- 21.↵
- 22.↵
- 23.↵
- 24.↵
- 25.↵
- 26.↵
- 27.↵
- 28.↵
- 29.↵
- 30.↵
- 31.↵
- 32.↵
- 33.↵
- 34.↵
- 35.↵
- 36.↵
- 37.↵
- 38.↵
- 39.↵
- 40.↵
- 41.↵
- 42.↵
- 43.↵
- 44.↵
- 45.↵
- 46.↵
- 47.↵
- 48.↵
- 49.↵
- 50.↵
- 51.↵
- 52.↵
- 53.↵
- 54.↵
- 55.↵
- 56.↵
- 57.↵
- 58.↵
- 59.↵
- 60.↵
- 61.↵
- 62.↵
- 63.↵
In this issue
Article tools






Jump to section
Related Articles
Cited By...
More in this TOC Section
Similar Articles

