


Sander DS, Carter MJ, Hurlstone DP, Pearce A, Ward AM, McAlindon ME, et al. Association of adult coeliac disease with irritable bowel syndrome: a case–control study in patients fulfilling Rome II criteria referred to secondary care. Lancet 2001;358:1504-8.
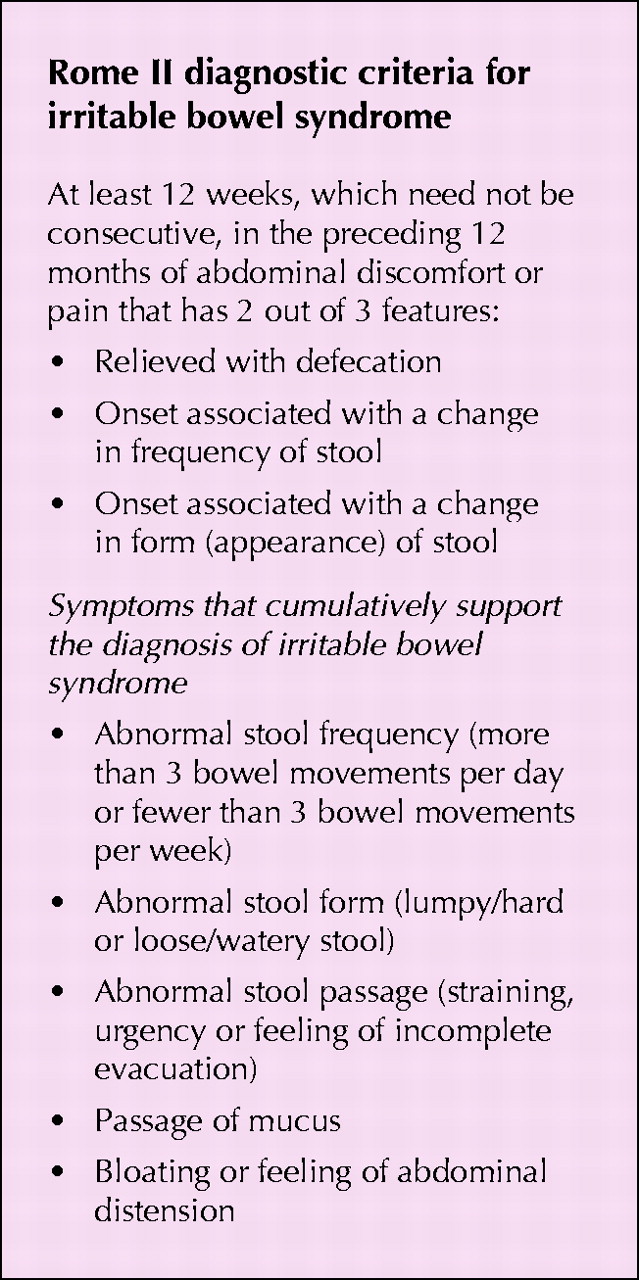
Background: Irritable bowel syndrome is common. It is found in 10% to 20% of people1,2 with the use of standard diagnostic tools such as the Rome II criteria3 (text box). The condition is twice as common in women as in men and can sometimes be difficult to distinguish clinically from celiac disease. Studies in Europe have shown that up to 1% of the adult population may have celiac disease.4,5 The recent development of serologic assays that have reasonable sensitivity and specificity for celiac disease have led to increased recognition that the disease is more common than was believed and may present with atypical or, indeed, no gastrointestinal symptoms. This explains the increased concern that some patients in whom irritable bowel syndrome has been diagnosed may in fact have celiac disease.
{kind=link}
Question: What proportion of patients who meet the Rome II criteria for irritable bowel syndrome have celiac disease?
Methods: The authors applied the Rome II criteria for irritable bowel syndrome to 686 new patients presenting to a university hospital gastroenterology clinic after referral by a family physician. None of the patients had had their condition investigated previously. A total of 300 people (214 women, 86 men) met the criteria; they ranged in age from 18 to 87 (mean 56) years.
Control subjects — healthy people without irritable bowel syndrome — were recruited from family practices in the hospital catchment area. Patients or their companions (most control subjects were companions) were invited to volunteer for the study while they were in the waiting rooms of their family doctors. Control subjects were matched to case subjects by age (within 1 year) and sex, and questioned in the same fashion as the case subjects.
All case and control subjects underwent a wide range of baseline investigations, including full blood count, measurement of erythrocyte sedimentation rate, blood urea nitrogen and serum electrolyte levels, and thyroid function tests. In addition, they were investigated for celiac disease by analysis of serum levels of IgG antigliadin, IgA antigliadin and endomysial antibodies. Most of the case subjects, particularly those older than 45, underwent colonoscopy or sigmoidoscopy and barium enema. Case and control subjects with positive antibody test results were offered duodenal biopsy to confirm the possibility of celiac disease.
Results: Of the 66 case subjects who had positive antibody test results, 49 had elevated levels of only IgG antigliadin, 4 of only IgA antigliadin and 6 of only endomysial antibodies. Fourteen of the 66 were subsequently found to have histologic evidence of celiac disease; 11 of the 14 were positive for endomysial antibodies. Nine of the 66 case subjects were lost to follow-up or refused duodenal biopsy; 1 of them was positive for endomysial antibodies.
Of the 44 control subjects who had positive antibody test results, 41 had elevated levels of only IgG antigliadin, 1 of only IgA antigliadin and 2 of IgG antigliadin and endomysial antibodies. Only the last 2 subjects elected to undergo duodenal biopsy, and both were found to have histologic evidence of celiac disease.
Commentary: The authors found that a high proportion of patients (about 5%) who were referred to a university hospital gastroenterology clinic and who met the Rome II criteria did have celiac disease. In addition, the clinic specialists uncovered other organic abnormalities in almost 20% of the referred patients.
The study had several weaknesses. For instance, although most of the case subjects underwent extensive investigations of the lower gastrointestinal tract, the control subjects did not. Thus, some of the case subjects who were lost to follow-up or refused investigation and many of the age-matched control subjects might have been found to have irritable bowel disease, celiac disease or other gastrointestinal abnormalities.
The authors conclude from their findings that patients who meet the Rome II criteria for irritable bowel syndrome and who are referred to a secondary care centre should be investigated routinely for celiac disease.
Implications for practice: Almost all primary care physicians and internists have seen and manage patients with irritable bowel syndrome. The difficulty has been in knowing how far to go with investigations to rule out organic causes of their symptoms. Celiac disease is more common than once was thought, and newer tools, especially endomysial antibody tests, are thought to be more specific than the widely used IgG and IgA antigliadin tests.
In an editorial accompanying the Lancet article a gastroenterologist cautioned that more studies are needed.6 He noted an earlier study in which 121 consecutive patients were referred for investigation of irritable bowel syndrome. Using Rome I criteria and similarly extensive investigations, the researchers detected no cases of celiac disease.6
Because of the findings from the Lancet study, the editorialist has decided to further lower his threshold for screening for celiac disease among patients referred for investigation of irritable bowel syndrome. Perhaps other gastroenterolgists would be wise to do the same.
John Hoey CMAJ
In this issue
Article tools






Jump to section
Related Articles
Cited By...
- No citing articles found.
More in this TOC Section
Similar Articles
Collections

