


A 41-year-old Japanese woman with a six-year history of ocular and pulmonary sarcoidosis had elevated levels of hepatobiliary enzymes, identified during a period health examination (Appendix 1, available at www.cmaj.ca/lookup/suppl/doi:10.1503/cmaj.180276/-/DC1). She had no abdominal symptoms or evidence of chronic liver disease, and she had not been taking steroids. Enhanced computed tomography (CT) showed hepatomegaly with multiple mottled low-density lesions (Figure 1A). A positron emission tomography/CT analysis showed diffusely increased hepatic uptake of 18F-fluorodeoxyglucose (FDG) (Figure 1B), and a subsequent liver biopsy showed an accumulation of noncaseating epithelioid granulomas with multinucleated giant cell invasion. We diagnosed hepatic sarcoidosis and prescribed a three-day methylprednisolone pulse of 1 g/d, followed by oral prednisolone 40 mg/d for a month. Because glucocorticoid therapy was only partially effective, we also administered adalimumab (Appendix 2 [Figure A], available at www.cmaj.ca/lookup/suppl/doi:10.1503/cmaj.180276/-/DC1). Subsequently, her liver function returned to normal, and imaging showed a reduction in hepatomegaly and a decrease in low-density areas (Appendix 2 [Figure B]). She has remained in remission for the past two years, with ongoing adalimumab monotherapy.
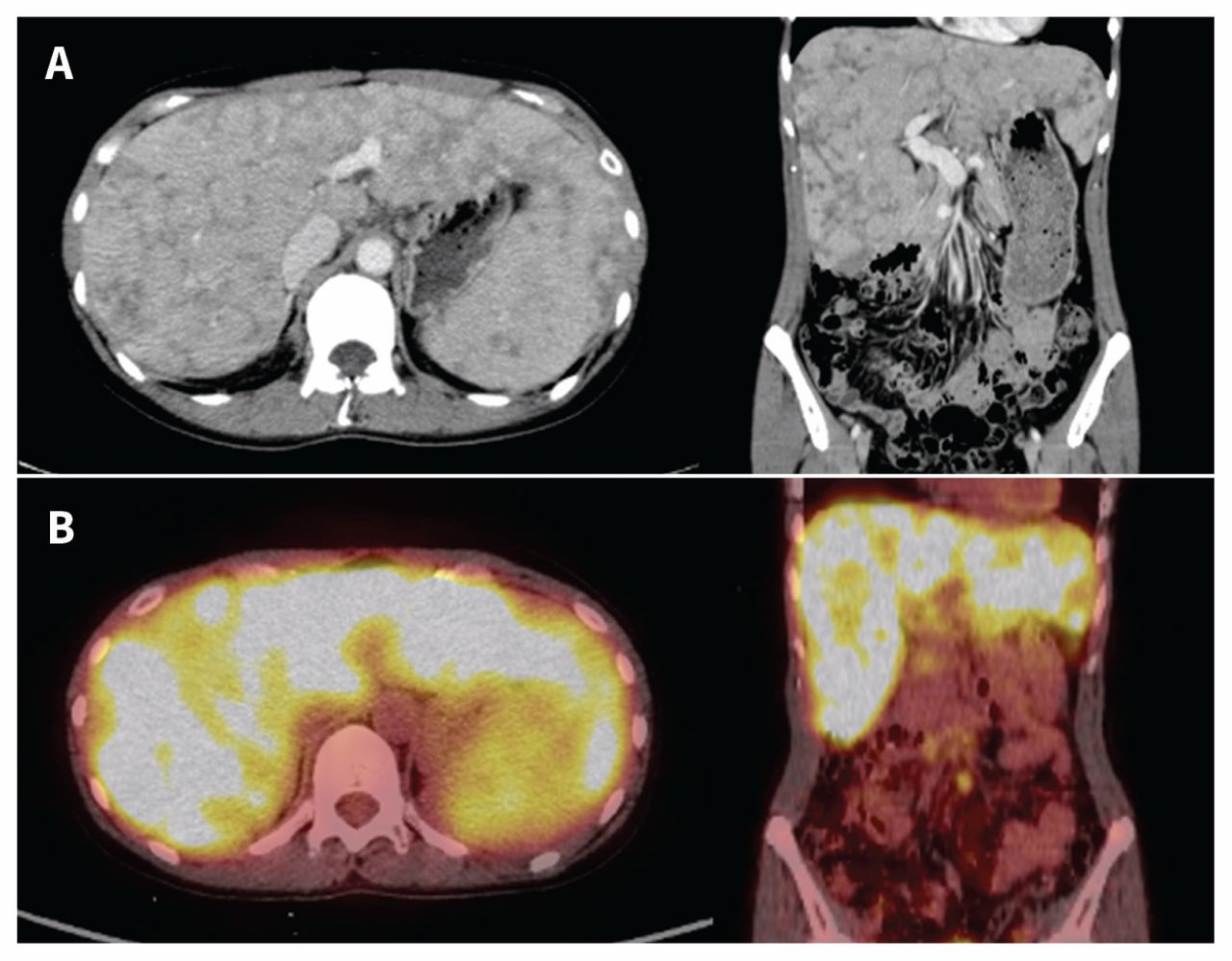
(A) Computed tomography (CT) scan of a 41-year-old Japanese woman with sarcoidosis showing hepatomegaly with multiple mottled low-density lesions. (B) 18F-fluorodeoxyglucose (FDG) positron emission tomography/CT showing the diffuse increment of 18F-FDG uptake in the patient’s liver.
Sarcoidosis is a systemic inflammatory disease of unknown etiology, which is characterized by noncaseating epithelioid granulomas. Sarcoidosis primarily affects the lungs and hilar lymph nodes. The heart, liver and spleen are often involved in extrapulmonary manifestations. Hepatic sarcoidosis has an estimated prevalence of 5%–30% in antemortem cohort studies and 70% in a postmortem study.1 Liver involvement is usually asymptomatic, with normal liver enzyme levels, and abdominal ultrasonography and CT are normal in almost 50% of patients with biopsy-proven hepatic sarcoidosis.1
Positron emission tomography/CT with 18F-FDG is a promising technique to evaluate metabolic activity and is widely accepted for use in detecting active sarcoid lesions.2 Expert consensus supports glucocorticoids as first-line therapy, with tumour necrosis factor inhibitors, including adalimumab, reserved for glucocorticoid-resistant cases.3
Footnotes
Competing interests: None declared.
This article has been peer reviewed.
The authors have obtained patient consent.
In this issue

{kind=link}
Article tools






Related Articles
Cited By...
- No citing articles found.
More in this TOC Section
Similar Articles
Collections

