


- © 2008 Canadian Medical Association
A 24-year-old woman was referred to our dermatology clinic for assessment of vulvar papules. They had been present for at least 2 years, during which time she had tried a course of imiquimod 5% cream, a wart treatment. The lesions, aside from causing significant embarrassment, had not changed in number or size and were asymptomatic. The patient had no known history of sexually transmitted infections. Examination revealed multiple tiny, filiform, rosy papules, symmetrically distributed on the inner sides of her labia minora (Figure 1). The papules were not spreading. The projections were easily separated from each other on examination. The affected area was not painful to touch.

Figure 1: Multiple symmetrical papules on the labia minora of a 24-year-old woman. The papules, present for at least 2 years, had not changed in number or size and were asymptomatic.
-
Genital warts (condylomata acuminata)
-
Vulvar intraepithelial neoplasia
-
Genital herpes
-
Vulvar papillomatosis
-
Condylomata lata (syphilis)
What is your diagnosis?
Discussion
The answer is (d) vulvar papillomatosis. This diagnosis is based on the case chronology, the stability of the lesions over time and the findings on clinical examination of discrete, symmetrical filiform papules on the vestibule.
Vulvar papillomatosis is a benign, asymptomatic anatomic variant of the vulvar epithelium present in about 1% of women.1 It is characterized by linear, pink, smooth or filiform papules symmetrically distributed on the inner surface of both labia minora.
Histologically, the lesions consist of acanthosis or papillomatosis without koilocytes or mitotic activity. The possible association of vulvar papillomatosis with human papillomavirus has lead to controversies about its cause.2,3
Genital warts (condylomata acuminata) are not confined to the vestibule. The filiform or cauliflower projections of condyloma tend to fuse at the base (Figure 2A).
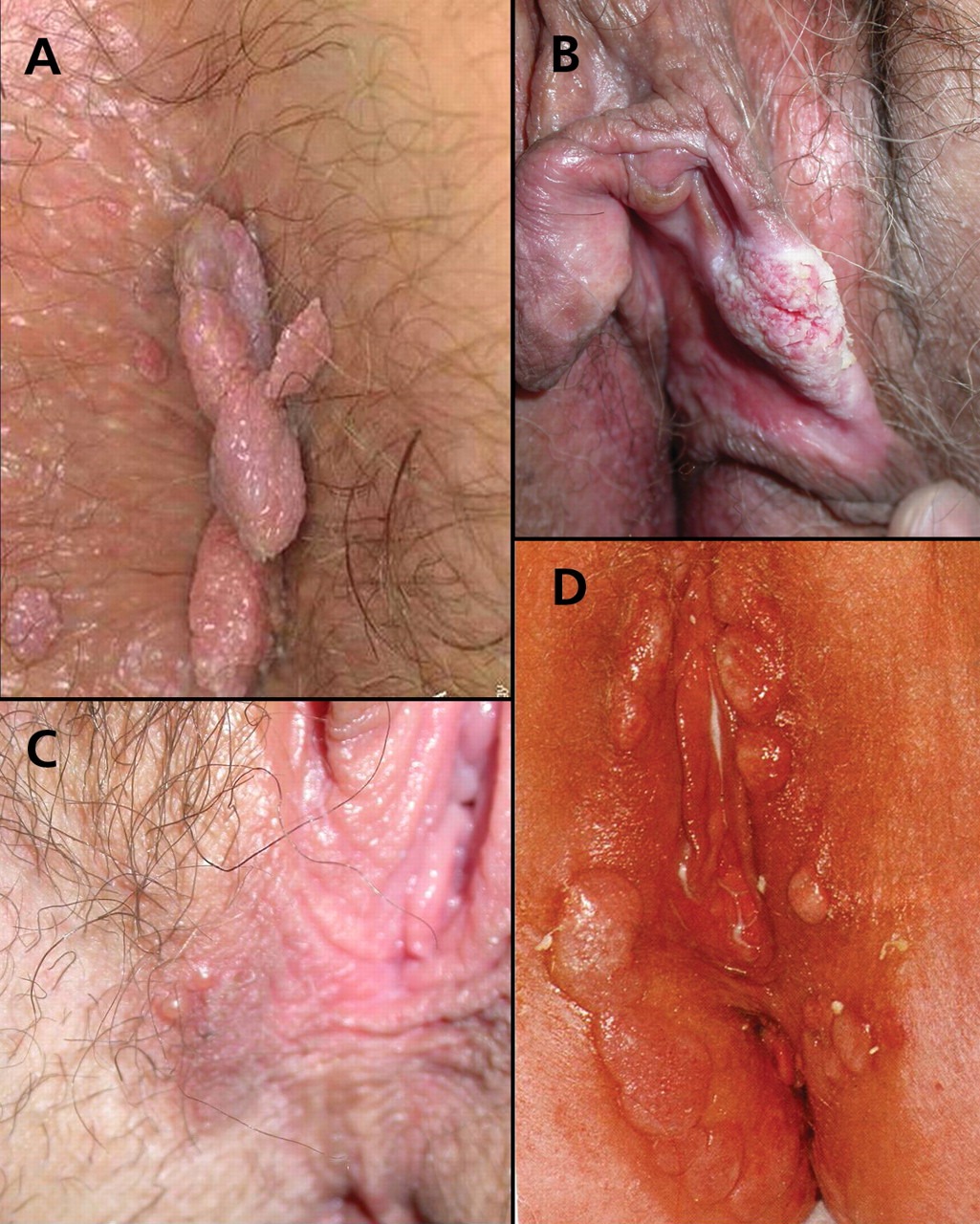
Figure 2: (A) genital warts, (B) vulvar intraepithelial neoplasia, (C) genital herpes, (D) condylomata lata.
Lesions of vulvar intraepithelial neoplasia (Figure 2B) are clinically variable and nonspecific. They closely resemble non-neoplastic epithelial abnormalities or shallow verrucocities. They may be dull red and granular, or they may present with a variegated red and white pigmented appearance with interspersed warty areas. The diagnosis can be made only by biopsy. In our case, we decided against biopsy because the clinical presentation was typical for benign disease: all of the papules were separate and symmetrically distributed, whereas neoplasia often presents as a unique patch.
Genital herpes (Figure 2C) may be preceded by 2 or 3 days of itching. The lesions themselves are at first erythematous. They rapidly become vesicular, and then rupture to form groups of shallow ulcers, 1–2 mm in diameter. Lesions can appear on any part of the genital region. The detection of circulating IgM antibodies against herpes simplex virus types 1 and 2 is used to confirm the diagnosis.
Condylomata lata (Figure 2D) are a variant of the papular syphilide (clinical features of secondary syphilis). They develop at the vulvar periphery (frequently on the labia majora) and around the anus. They appear as confluent soft spongy masses with flat tops and broad bases. The lesions tend to be painless. They can become eroded and exude infective serum. Results of serologic tests for syphilis (Venereal Disease Research Laboratory test and Treponema pallidum hemagglutination assay) are positive.
Knowledge of anatomic variants of vulvar epithelium such as vulvar papillomatosis allows patients to be appropriately reassured and helps to prevent further unnecessary investigations.
Footnotes
-
CMAJ invites submissions to “What is your call?” Clinical details (including images) are presented on the first page along with a multiple-choice question about the diagnosis. The answer and a brief discussion of the condition follow on the second page. We specifically invite submissions illustrating common or important radiographic and electrocardiographic diagnoses of appeal to a general audience. We allow up to 5 references and require authors to obtain consent from the patient for publication of his or her story (form available at www.cmaj.ca/authors/checklist.shtml). Submit manuscripts online at http://mc.manuscriptcentral.com/cmaj.
This article has been peer reviewed.
Competing interests: None declared.
In this issue

{kind=link}
{kind=link}
Article tools






Related Articles
Cited By...
- No citing articles found.
More in this TOC Section
Similar Articles
Collections

