


A 78-year-old man presented for follow-up of transient ischemic attacks (TIAs) that occurred in 1990 and 1992 in the right carotid territory; he had been asymptomatic since that time. He was a smoker and had hyperlipidemia, hyperhomocysteinemeia (19.9 [target < 10] μmol/L)1 and a high level of lipoprotein(a) (0.4 [normally < 0.2] g/L). He was taking daily simvastatin (40 mg), ASA (325 mg), folic acid (2.5 mg), pyridoxine (25 mg), cyanocobalamin (500 μg) and a multivitamin tablet; for reasons of inconvenience he had recently stopped taking niacin, which had been prescribed because of his high lipoprotein(a) level. His heart rate and blood pressure were normal, and his fasting lipid profile showed a total cholesterol level of 4.46 mmol/L, triglycerides 0.96 mmol/L, high-density lipoprotein (HDL) cholesterol 0.97 mmol/L and low-density lipoprotein (LDL) cholesterol 3.4 mmol/L. He had known stenosis of 70% in the right internal carotid artery, with diffuse atheroma in the carotids.
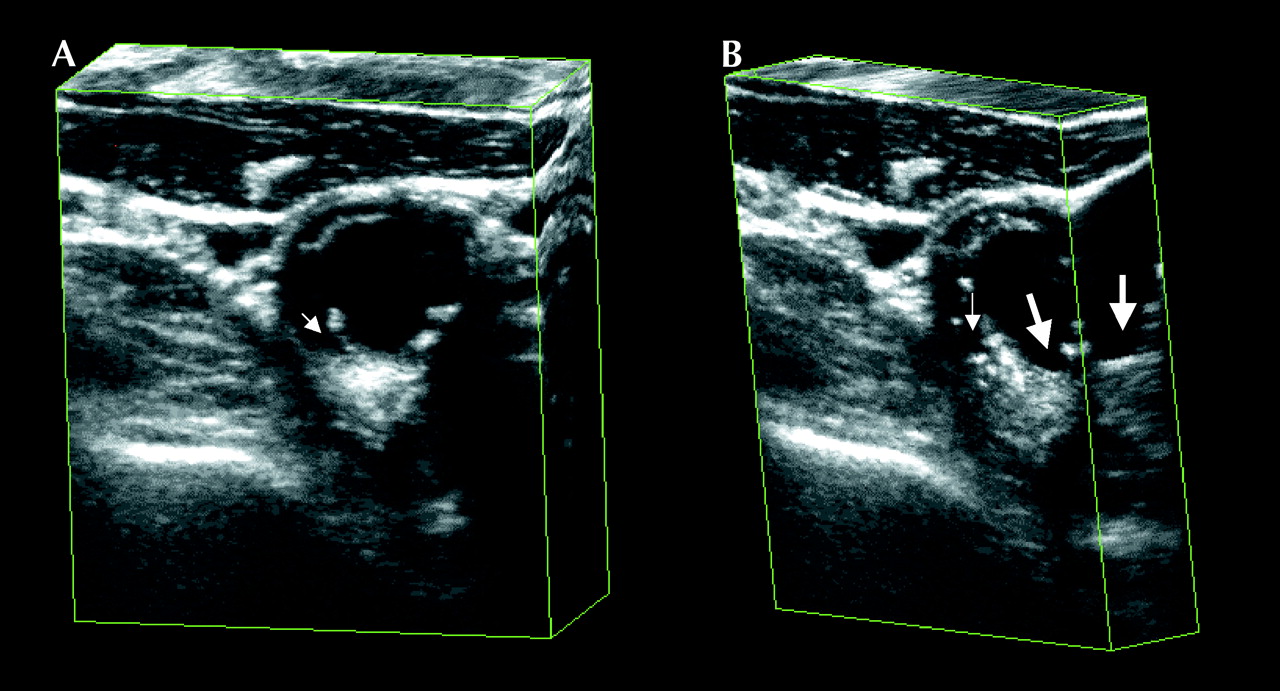
Because the TIAs were so remote in time, the man's risk of further cerebral ischemic events had fallen to a level equivalent to that of asymptomatic stenosis.2 Furthermore, during the previous 2 years the carotid plaque area had regressed from 3.85 cm2 to 3.0 cm2 after the addition of folate, pyridoxine and cyanocobalamin for hyperhomocysteinemia,1 another indication that his risk of cerebral events may be low. To evaluate whether his carotid plaque was unstable, he underwent 1 hour of transcranial Doppler monitoring of the middle cerebral arteries, aimed through the thinnest part of the temporal bone: 2 microemboli were detected. Three-dimensional ultrasonography of the right carotid artery (Figs. 1A and 1B) indicated multiple ulcers (thick arrows) and fissures (thin arrows) of the stenotic lesion, the likely source of the microemboli. Lung cancer was diagnosed soon after these studies were performed, and the patient decided to delay carotid endarterectomy. A year later he has had no further TIAs or strokes. His medical therapy has been unchanged.

{kind=link}
Figure 1. Photo: Courtesy: J. David Spence
Although endarterectomy is an effective treatment of symptomatic severe carotid stenosis,2 it is not routinely warranted in asymptomatic cases.3 Patients with severe symptomatic carotid stenosis have on average 6 microemboli per hour, which disappear with endarterectomy.4 The presence of microemboli, which has been associated with an 8-fold risk of subsequent cerebral events in both symptomatic and asymptomatic patients,5 may justify endarterectomy in asymptomatic patients.
J. David Spence Arturo Tamayo Maria DiCicco Stroke Prevention and Atherosclerosis Research Centre The John P. Robarts Research Institute London, Ont.
In this issue
Article tools






Jump to section
Related Articles
Cited By...
- No citing articles found.
More in this TOC Section
Similar Articles

