


Abstract
Background: There are concerns about the frequency and appropriateness of psychostimulant drug prescription to children. In order to identify unusual or unexpected patterns of use or prescribing, we reviewed prescription of methylphenidate (Ritalin) to children and adolescents aged 19 years or less in British Columbia between 1990 and 1996.
Methods: We obtained information about patients, physicians and prescriptions from British Columbia's Triplicate Prescription Program database for controlled drugs. Prescription data were available for the period Jan. 1, 1990, to Dec. 31, 1996. Linkage with the BC Linked Health Dataset provided additional demographic and health information.
Results: In 1990, 1715 children received at least 1 prescription for methylphenidate (1.9 per 1000 children). By 1996, the number had increased to 10 881 children (11.0 per 1000). Because some children were prescribed methylphenidate in more than 1 year, we also calculated the frequency with which the drug was prescribed to children who had never received it before. This rate increased from 1.0 per 1000 children in 1990 to 4.7 per 1000 in 1995; the rate fell in 1996 to 3.5 per 1000. The number of children receiving methylphenidate varied across health regions of the province, from 12.0 to 35.4 per 1000. Use also varied by socioeconomic status quintile: in the 2 lowest (least privileged) quintiles, 21.6 per 1000 children received methylphenidate, compared with 18.4 per 1000 in the 3 highest quintiles (relative risk 1.2, 95% confidence interval 1.1–1.2). Pediatricians and psychiatrists wrote 23% and 21% of all prescriptions respectively. General practitioners accounted for 56% of all prescriptions and 41% of initial methylphenidate prescriptions. A claim for prior specialist consultation was found in 30% of such cases. Many of the children who received more than 10 prescriptions had seen 4 or more physicians. The average daily dosage prescribed differed little among general practitioners, pediatricians and psychiatrists, unlike the mean interval between successive prescriptions: 89.9 (standard deviation [SD] 68.2), 99.8 (SD 64.1) and 75.9 (SD 70.2) days respectively. Persistence with therapy was more likely when a psychiatrist provided the initial prescription, or with involvement of more than one specialty.
Interpretation: Many trends and practices in the prescription of methylphenidate to children in British Columbia are consistent with other settings and accepted standards. Some aspects warrant closer investigation, including regional and socio-economic discrepancies in the distribution of patients, the relative involvement of primary and specialist care providers, continuity of care issues and time intervals between prescriptions.
Methylphenidate (Ritalin) is the psychostimulant drug that is most frequently prescribed in the management of attention-deficit hyperactivity disorder (ADHD),1,2 a behavioural syndrome estimated to affect 3%–5% of school-aged children.3 Marked increases in rates of prescription of psychostimulants to children during the 1990s, best documented in the United States2,4 but also noted by media and industry sources in Canada5 (Dorothy Rhodes, Senior Analyst, Corporate Relations and Development, IMS HEALTH Canada, Montreal: personal communication, 1999) have resulted in public health concerns about the frequency and appropriateness with which these medications are prescribed to children.1,2,6 Expert consensus and emerging research evidence highlight the need for comprehensive initial diagnostic assessment when ADHD is suspected, tailoring of treatment to individual needs, multimodal and multidisciplinary approaches, careful titration of stimulant medication, and close follow-up and monitoring of children receiving medication.7,8,9,10,11,12,13 However, deficiencies have been reported in the way that physicians in the United States assess and manage children presenting with features of ADHD.9,14,15 The few studies of Canadian physicians are limited by poor response rates and a lack of independent validation of responses.16,17
The existence of universal coverage for medical care in Canada and the availability of administrative prescription and health databases in certain provinces permit population-based research to address methylphenidate use and practice patterns in a Canadian setting. We performed a study to identify unusual or unexpected patterns of use and prescribing of methylphenidate, through a series of analyses of linked administrative prescription and health databases in British Columbia.
Methods
Children and youth aged 19 years or less who received at least 1 prescription for methylphenidate were identified from BC's Triplicate Prescription Program database for controlled drugs. Patient age was determined as age at the time of the first prescription. Available data included each patient's Personal Health Number (a unique personal identifier assigned to residents of the province whose needs for medically necessary services are universally insured through the government-run Medical Services Plan), drug preparation type (brand name or generic), tablet strength and quantity, date dispensed and a unique prescribing physician identifier. The range of data available for patients and physicians was extended though linkage with the BC Linked Health Dataset, developed and maintained by the Centre for Health Services and Policy Research at the University of British Columbia, Vancouver, in collaboration with the BC Ministry of Health.
The dataset contains person-specific demographic and health service use records of Medical Services Plan clients.18 We obtained information, including specialty type, for all physicians licensed in the province during 1990–1996 from a subsidiary file, the Medical Services Plan Practitioner File. Linkages are made possible by the use of common personal identifiers in the prescription database and the BC Linked Health Dataset. Encryption procedures applied to these identifiers ensured confidentiality of the information collected. We obtained estimates of population size by age group for individual study years from BC STATS.19
Access to nonidentifying data for individuals was granted by the Ministry of Health under its access policy. The project was approved by the Research Ethics Review Board of the University of British Columbia and the College of Physicians and Surgeons of BC.
The population of BC was about 3.7 million at the midpoint of the study,19 served by approximately 4300 general practitioners (GPs), 220 pediatricians and 450 psychiatrists,17,20 including an estimated 50 child psychiatrists. Most physicians are paid on a fee-for-service basis through the Medical Services Plan,21 based on specialty and service-specific fee schedules. GPs provide most primary care received by children and youth, with pediatricians and psychiatrists providing mainly consultative services.
Prescription data were available for the period from Jan. 1, 1990, to Dec. 31, 1996. Between September 1995 and December 1996, methods of capturing Triplicate Prescription Program data changed, and audits from this period showed some errors in the coding of the identity of prescribing physicians. Therefore, for analyses involving physician specialty type, we elected to include data only from the period for which accuracy was more assured (January 1990 to August 1995).
We determined the prevalence of methylphenidate use in individual years as the number of patients who received 1 or more prescriptions for the drug in a study year, irrespective of prescription history in previous years, per 1000 children and youth in the general population. Prevalence estimates for the periods 1990–1996 and January 1990 to August 1995 were calculated as a count of all cases over the time period, divided by the averaged population estimate for each time period. Incidence (the number of patients who received their first recorded prescription during the study period) was determined for each study year. Children and youth who received prescriptions over at least a 12-month period, with no interval between prescriptions longer than 4 months, were designated as long-term users.
There are 20 administrative health regions in British Columbia. The patient's health region was deemed to be that in which he or she resided at the time of the first prescription.
Indicators of socioeconomic status included family socioeconomic status quintile, based on neighbourhood of residence (using a method that ranks neighbourhoods by average income adjusted for household size)22 and receipt of a subsidy toward payment of health care insurance premiums. Because subsidies are provided based on economic need, receipt of a subsidy was taken to indicate lower socioeconomic status.
To determine features of therapy, we used data from the fifth prescription on the assumption that titration would be complete and stability would be achieved by that time. We estimated the daily dosage level for an administration schedule of 7 days per week from the number of tablets prescribed in the fifth prescription, multiplied by tablet strength, divided by the number of days to the subsequent prescription.23 The interval between prescriptions was defined as the number of days that elapsed between the filling of the fifth and sixth prescriptions.
Results
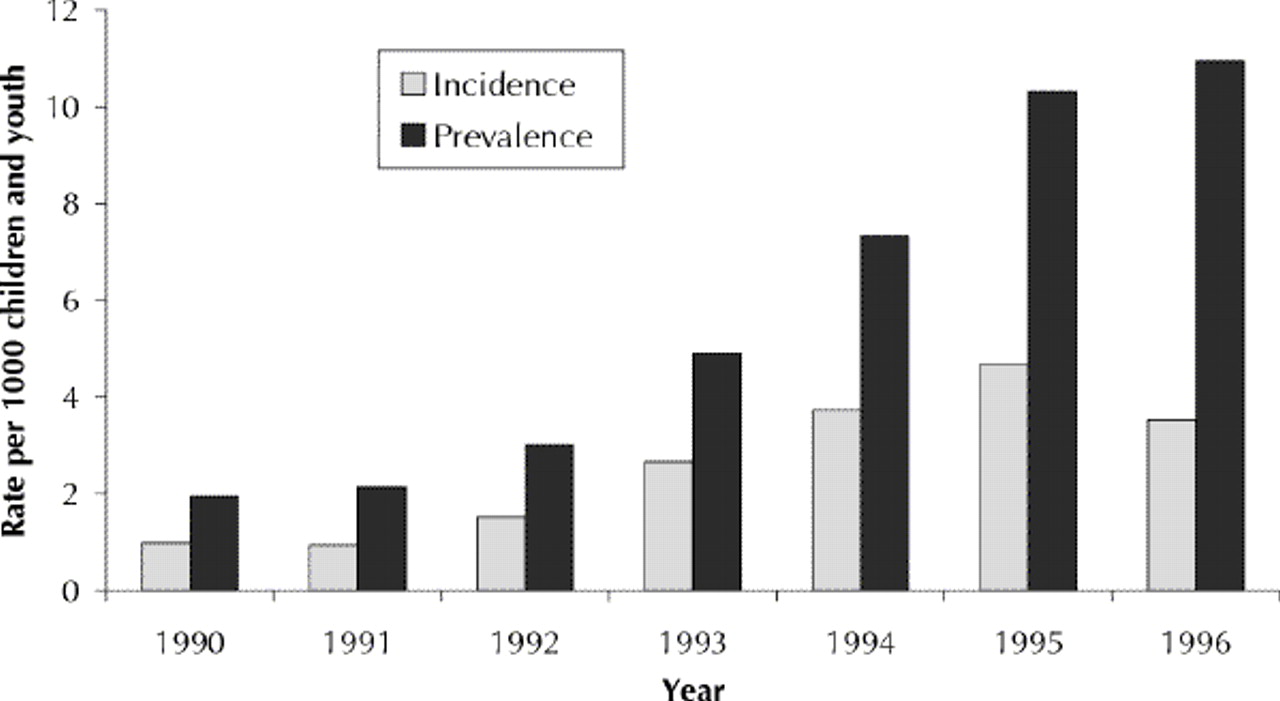
A total of 134 036 prescriptions for methylphenidate were filled for 18 081 children and youth in 1990–1996. The prevalence of use quintupled over the study period, from 1.95 per 1000 in 1990 to 10.96 per 1000 in 1996 (Fig. 1). The incidence increased from 0.99 per 1000 in 1990 to 4.67 per 1000 in 1995, and then declined slightly to 3.52 per 1000 in 1996.
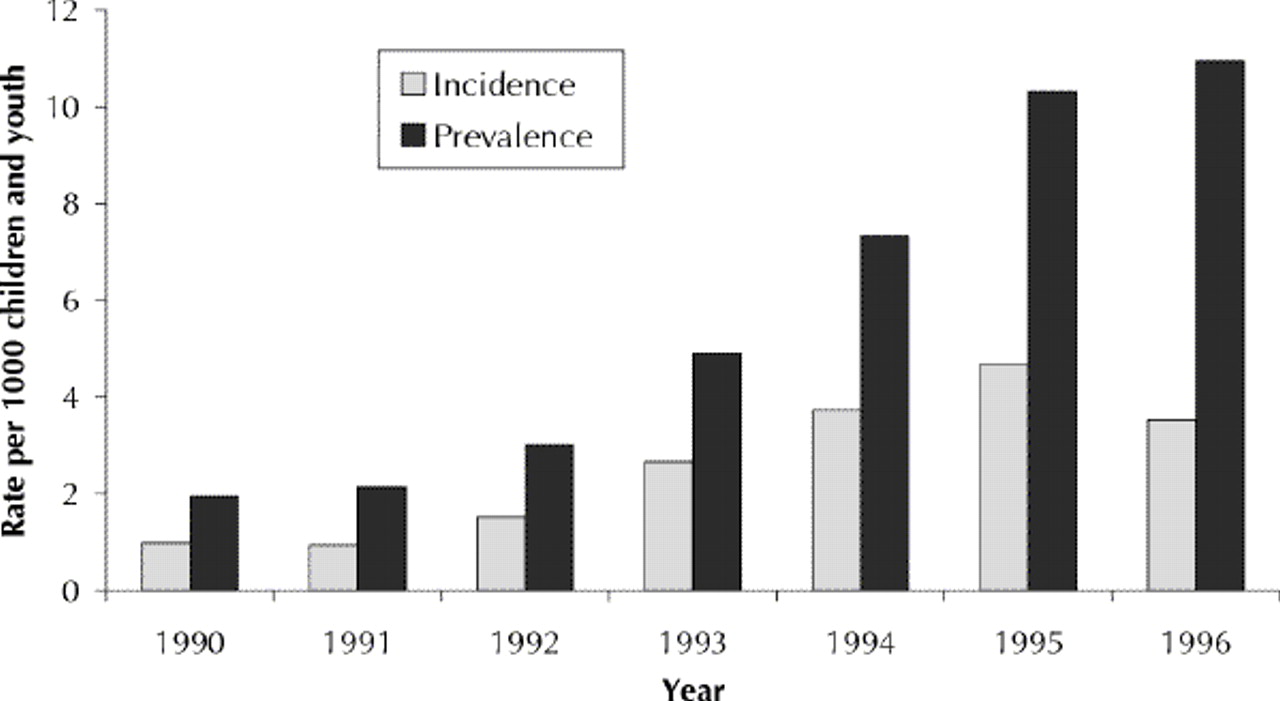
Fig. 1: Incidence and prevalence of methylphenidate use in children and youth aged 19 years or less in British Columbia, 1990–1996.
Patient characteristics
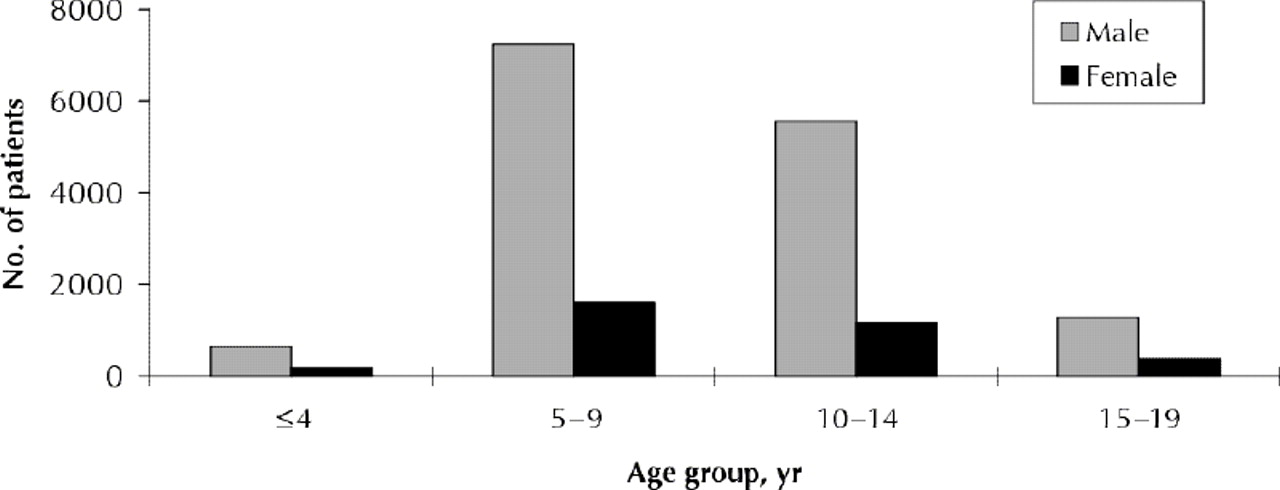
Of the 18 081 children and youth, 14 731 (81.5%) were boys, most aged 5–14 years (Fig. 2). The average age at the time of the first prescription was 9.6 years, with a slight incremental trend from 9.2 years in 1990 to 9.7 years in 1996.

Fig. 2: Methylphenidate use by age and sex.
There was considerable variability in the overall prevalence of use of methylphenidate across health regions, ranging from 12.05 to 35.45 per 1000 children and youth, with a provincial mean of 19.3 per 1000. Use of the drug was slightly higher among children and youth in the lowest 2 (least privileged) socioeconomic quintiles than in the highest 3 quintiles (21.6 v. 18.4 per 1000 children and youth) (relative risk 1.17, 95% confidence interval 1.14–1.21). Health care premium subsidy status was known for 93.3% of the 1.52 million children and youth aged 19 years or less in the province. Methylphenidate use was higher among children and youth whose families had received a subsidy than among those whose families had not (14.2 v. 11.2 per 1000 children and youth) (relative risk 1.27, 95% confidence interval 1.22–1.30).
Characteristics of prescribing physicians
GPs, pediatricians and psychiatrists wrote 55.5%, 23.3% and 20.6% respectively of the prescriptions. A total of 62% of the GPs registered in the province, 52% of the pediatricians and 27% of the psychiatrists wrote at least 1 prescription for methylphenidate for a child or youth during the study period. For children and youth who persisted with therapy, the responsibility for prescribing shifted over time (Fig. 3). GPs wrote 40.6% of first prescriptions, pediatricians 38.5% and psychiatrists 20.1%. The proportion of prescriptions written by GPs increased to 58.2% for fifth prescriptions and 67.0% for tenth prescriptions, whereas the proportion written by pediatricians decreased to 24.2% and 17.5% respectively and the proportion written by psychiatrists decreased to 17.5% and 15.5% respectively. Among the children and youth who received their initial prescription from a GP, a fee claim for a specialist consultation with a pediatrician, psychiatrist or neurologist in the 6 months before the prescription was found in 29.7% of cases.
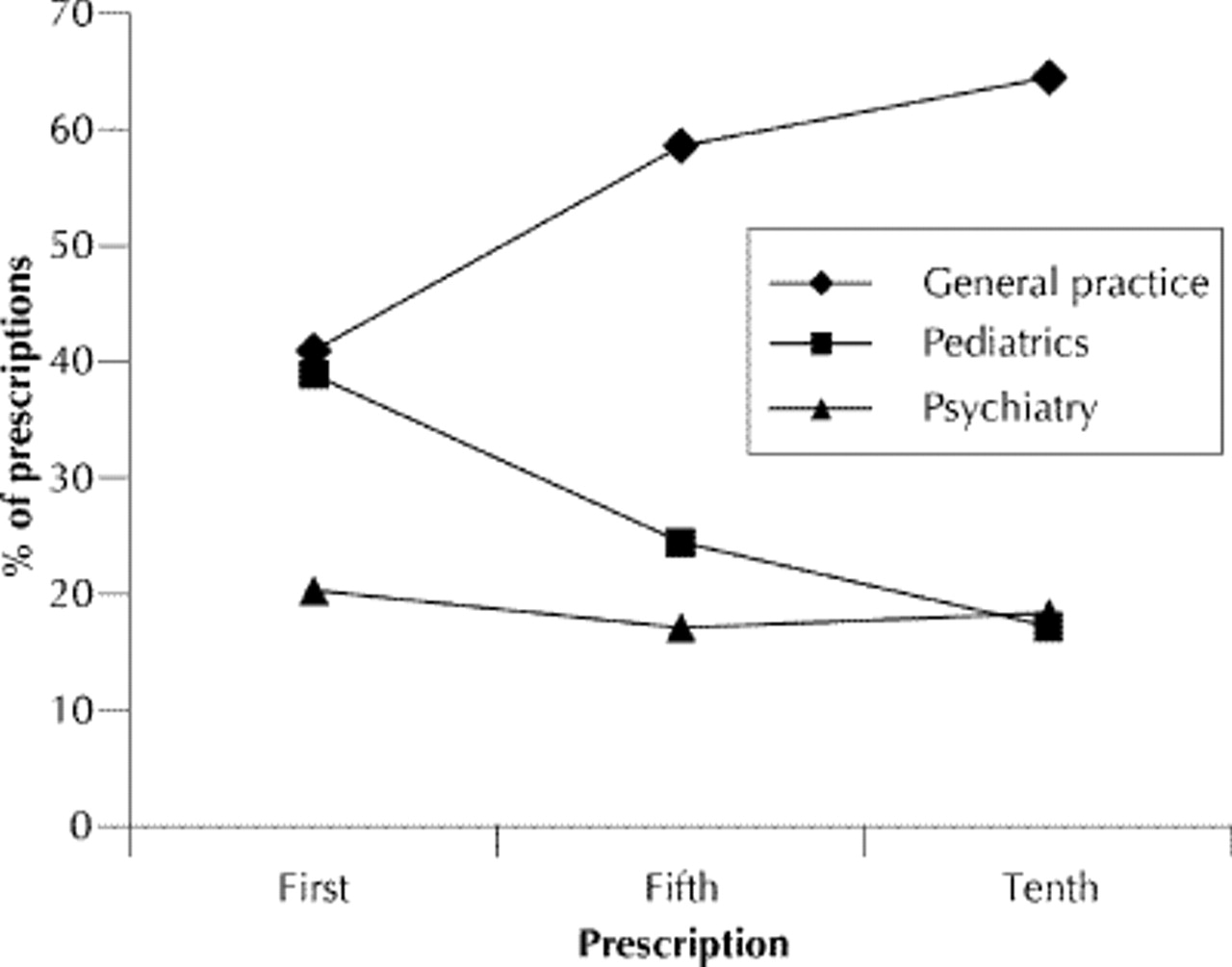
Fig. 3: Specialty of physicians writing first, fifth and tenth prescriptions.
Continuities and discontinuities in physicians' prescribing role
The vast majority (87.1%) of children and youth received their second prescription of methylphenidate from a physician of the same specialty that provided the first. In most cases (77.9%) in which specialty crossover did occur, a specialist wrote the first prescription and a generalist wrote the second. This occurred in about 18% of cases in which therapy was initiated by a pediatrician or psychiatrist.
In the period from January 1990 to August 1995, children and youth who received fewer than 5 prescriptions tended to receive them from at most 2 physicians, whereas many of the children and youth who received more than 10 prescriptions received them from 4 or more physicians (Fig. 4). Furthermore, in cases in which only 1 specialty was involved in care, 83.5% of patients received 5 or fewer prescriptions over the study period; in cases in which 2 or more specialty types were involved, 65.5% of patients received more than 6 prescriptions.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
Fig. 4: Number of prescribing physicians by number of prescriptions received.
Features of therapy and persistence with therapy
There was little difference in the mean daily dosage prescribed by GPs, pediatricians and psychiatrists (20.8 mg [standard deviation (SD) 15.1 mg], 20 mg [SD 13.8 mg] and 22.1 mg [SD 16.2 mg] respectively).The average daily dosage across specialty types was 20.2 mg (SD 14.5 mg). Pro-rating up by 1.4 (i.e., 7/5) gives an average daily dosage of 28.3 mg (SD 17.1 mg) for an administration schedule of 5 days per week. The interval between prescriptions, on the other hand, differed among specialties. The average interval between filling of the fifth and sixth prescriptions, when both were written by a physician of the same specialty, was 89.9 (SD 68.2) days for GPs, 99.8 (SD 64.1) days for pediatricians and 75.9 (SD 70.2) days for psychiatrists. A notably shorter interprescription interval of 70.1 (SD 44.4) days was found for long-term users.
Persistence with therapy appeared to be related to physician specialty: the ratio of children and youth who received more than 6 prescriptions relative to a single prescription varied with the specialty of the physician responsible for the child's or youth's initial prescription (p < 0.001) and was significantly higher for psychiatrists than for the other 2 specialty types (p < 0.001).
Interpretation
Rates of prescription of methylphenidate to children and youth in BC during the 1990s increased more rapidly than rates in the United States,4 but the 1995 prevalence figures of 2.5%–3% for US children4 remain considerably higher than the rate of 1.3% observed in BC. The downturn in the incidence of children receiving a prescription of methylphenidate after 1995 observed in BC is intriguing. Industry data show that this downturn coincides with a trend toward increased prescription of the psychostimulant dextroamphetamine (Dorothy Rhodes, Senior Analyst, IMS HEALTH Canada, Montreal: personal communication, 2000). Reassuring study findings were as follows: the age and sex distribution of children who received methylphenidate were consistent with the literature;4,24,25,26 there were no major discrepancies in dosage schedules used across the 3 main prescribing specialties; and there was a gradual and appropriate devolution of prescribing responsibility from specialists to GPs over the course of therapy.27 Findings that merit further attention are the following: the relative degree of involvement of primary and specialist care providers with this clinical population; regional and socioeconomic discrepancies in the distribution of patients; continuity of care issues; and interprescription intervals.
We examined grouped data that had not been collected for purposes of evaluative research. Hence, inferences about appropriateness of prescribing are not possible at the individual level, and our findings should be interpreted with caution overall. However, administrative database analysis allowed us to identify prescribing trends and practices that are consistent with other settings and accepted standards. Our analyses also revealed aspects of practice that merit further investigation.
The regional variations in the prevalence of methylphenidate prescription that we observed are consistent with findings from other settings;2,25,28,29 however, the causes of these variations remain unexplained.30 The combined effects of demographic, social, educational and medical services factors probably play a role. The relation between methylphenidate use and socioeconomic disadvantage is also difficult to interpret but may reflect the association of socioeconomic disadvantage with mental health problems in general31,32 and conduct disorders in particular.33,34 Future research should examine whether physicians preferentially use medication over other interventions when managing ADHD in disadvantaged children and should ensure that methylphenidate is not used inappropriately to manage aggressive behaviour and conduct disorders in the absence of ADHD.
The number of different physicians who became involved with prescribing to children with more than 1 prescription raises concerns, because continuity of care confers benefits in the management of chronic conditions.35 In addition, the transfer of prescribing responsibility from specialist to GP after just 1 prescription in 18% of cases raises questions about how adequately the important titration and stabilization phase was accomplished.
Practice guidelines for the management of ADHD do not state how frequently follow-up visits should be scheduled or for how long children should receive methylphenidate. Given the demonstrated benefits of highly structured titration and frequent follow-up, however,12,13 the intervals of 3 months between successive prescriptions that we observed for specialty types other than psychiatry seem to be at or beyond the upper limits of “best practice.” Most children who obtain benefit from stimulants require treatment over several years,36 and close to 80% of children with ADHD respond to methylphenidate with careful and individualized attention to dosage and administration.37 Hence, one indicator of quality of care would be a steeper, rather than flatter, ratio of children who persist with therapy rather than receiving a single prescription only.
In some parts of the world, management of children with ADHD is considered to require specialist involvement and, frequently, interdisciplinary collaboration.10,38 This potentially contentious issue remains largely unaddressed in Canada and the United States, although published guidelines for ADHD lay out standards for practice that are exacting and time-consuming.7,8,9,10,11 In addition, medication management characterized by meticulous titration and monitoring of medication effects and regular (monthly) follow-up visits has recently been shown to be associated with better outcomes than routine community-based care, even when the latter included medication.12,13 Our findings suggest that most GPs in BC have only sporadic exposure to children and youth with ADHD. Lack of exposure, training and time within current fee-for-service constraints presents considerable obstacles to primary care management of ADHD.6,8 Brief and superficial assessments are likely to lead to some children and youth receiving inappropriate prescriptions for methylphenidate or not being referred for other, appropriate interventions. The extent of GP- initiated methylphenidate therapy, without evidence of specialist consultation, is therefore of concern, even considering that our analyses may have missed a small amount of specialist care provided outside the fee-for-service system. However, there will probably never be a sufficient number of specialists to meet the needs of children and youth with developmental, behavioural and emotional problems.39 Therefore, health policy should aim to promote innovation at the level of the health services delivery system, enabling primary care physicians to provide care to this population at a level consistent with the expectations of existing practice guidelines.
Acknowledgments
We thank Harold Yip for programming, providing statistical analysis and producing summary tables for the project; Dorothy Rhodes, of IMS Canada, for generously making available her time and data; and Anne Klassen for reviewing an earlier version of the manuscript.
This work was supported by a grant from the BC Health Research Foundation. Dr. Miller is supported by an Investigator Award from the Sunny Hill Foundation for Children.
Footnotes
-
This article has been peer reviewed.
Competing interests: None declared.
References
In this issue
Article tools






Jump to section
Related Articles
Cited By...
- Prevalence, determinants and spectrum of attention-deficit hyperactivity disorder (ADHD) medication of children and adolescents in Germany: results of the German Health Interview and Examination Survey (KiGGS)
- Capacity and competence in children as research participants: Researchers have been reluctant to include children in health research on the basis of potentially naive assumptions
- Prevalence of methylphenidate use among Canadian children following parental divorce
- Evaluating potentially aberrant outpatient prescriptions for extended-release oxycodone
More in this TOC Section
Similar Articles

